

Three-Year Overall Survival with Durvalumab after Chemoradiotherapy in Stage III NSCLC-Update from PACIFIC
- PMID: 31622733
- PMCID: PMC7244187
- DOI: 10.1016/j.jtho.2019.10.002
Three-Year Overall Survival with Durvalumab after Chemoradiotherapy in Stage III NSCLC-Update from PACIFIC
Abstract
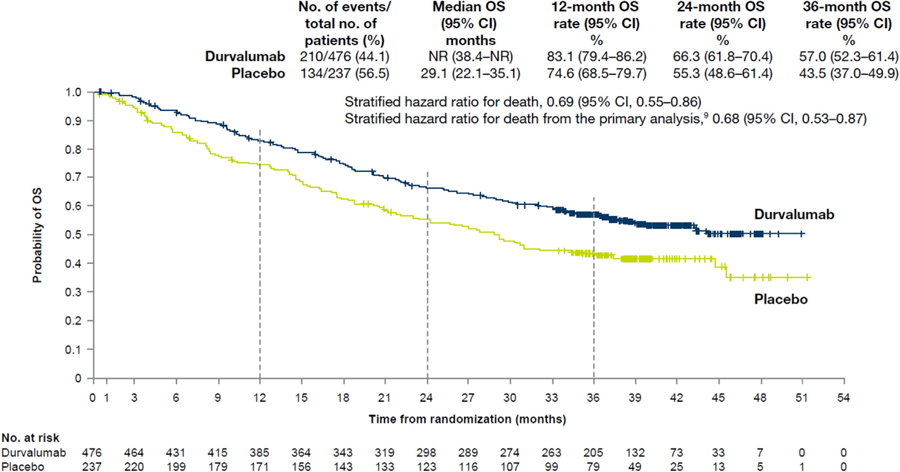
Introduction: In the phase 3 PACIFIC study of patients with unresectable stage III NSCLC without progression after chemoradiotherapy, durvalumab demonstrated significant improvements versus placebo in the primary end points of progression-free survival (hazard ratio [HR] = 0.52, 95% confidence interval [CI]: 0.42-65, p < 0.0001) and overall survival (OS) (HR = 0.68, 95% CI: 0.53-0.87, p = 0.00251), with manageable safety and no detrimental effect on patient-reported outcomes. Here, we report 3-year OS rates for all patients randomized in the PACIFIC study.
Methods: Patients, stratified by age, sex, and smoking history, were randomized (2:1) to receive durvalumab, 10 mg/kg intravenously every 2 weeks, or placebo for up to 12 months. OS was analyzed by using a stratified log-rank test in the intention-to-treat population. Medians and rates at 12, 24, and 36 months were estimated by the Kaplan-Meier method.
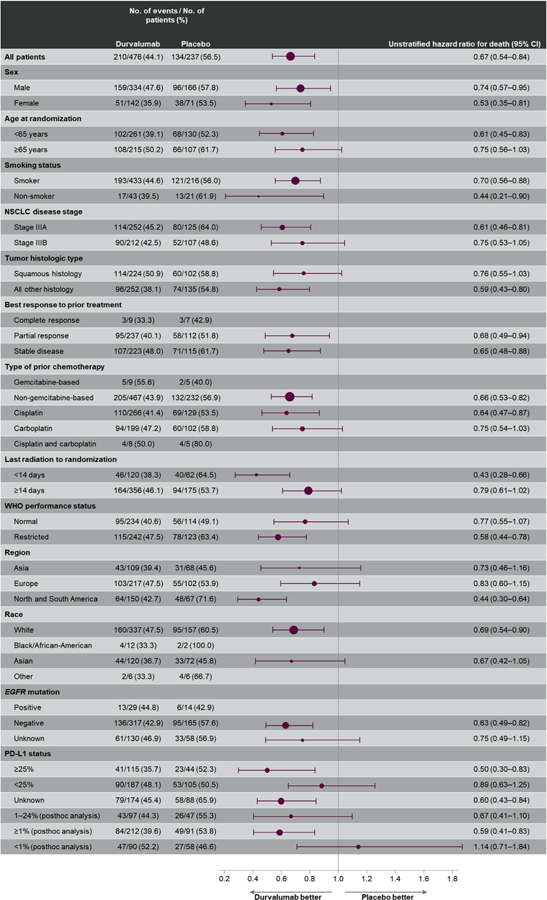
Results: As of January 31, 2019, 48.2% of patients had died (44.1% and 56.5% in the durvalumab and placebo groups, respectively). The median duration of follow-up was 33.3 months. The updated OS remained consistent with that previously reported (stratified HR = 0.69 [95% CI: 0.55-0.86]); the median OS was not reached with durvalumab but was 29.1 months with placebo. The 12-, 24- and 36-month OS rates with durvalumab and placebo were 83.1% versus 74.6%, 66.3% versus 55.3%, and 57.0% versus 43.5%, respectively. All secondary outcomes examined showed improvements consistent with previous analyses.
Conclusions: Updated OS data from PACIFIC, including 3-year survival rates, demonstrate the long-term clinical benefit with durvalumab after chemoradiotherapy and further establish the PACIFIC regimen as the standard of care in this population.
Trial registration: ClinicalTrials.gov NCT02125461.
Keywords: Durvalumab; NSCLC; Overall survival; PACIFIC; Three-year update.
Copyright © 2019 International Association for the Study of Lung Cancer. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Disclosure: Dr. Gray has received research funding, honoraria, and advisory fees from AstraZeneca. Dr. Villegas has received honoraria from AstraZeneca, Gilead, and Seattle Genetics. Dr. Daniel has received institutional research funding from E.R. Squibb and Sons, AstraZeneca, Boehringer Ingelheim, Genentech, Eli Lilly and Company, Novartis Pharmaceuticals, Pfizer, Celgene, and Roche. Dr. Hui has received advisory fees and honoraria from AstraZeneca, Merck Sharp and Dohme, Novartis, Roche, Bristol-Myers Squibb, and Eli Lilly and Company. Dr. Kurata has received research funding and honoraria from AstraZeneca. Dr. Chiappori has received speaker bureau funding from Genentech, Merck, Takeda, Novartis, Boehringer Ingelheim, and Celgene and research funding from Novartis and Bristol-Myers Squibb. Dr. Planchard has received advisory or lecture fees from AstraZeneca, Bristol-Myers Squibb, Boehringer Ingelheim, Celgene, Daiichi Sankyo, Eli Lilly, Merck, MedImmune, Novartis, Pfizer, prIME Oncology, Peer CME, and Roche; honoraria from AstraZeneca, Bristol-Myers Squibb, Boehringer Ingelheim, Celgene, Eli Lilly and Company, Merck, Novartis, Pfizer, prIME Oncology, Peer CME, and Roche; institutional research funding from AstraZeneca, Bristol-Myers Squibb, AbbVie, Boehringer Ingelheim, Eli Lilly and Company, Merck, Novartis, Pfizer, Roche, Medimmune, Sanofi-Aventis, Taiho Pharma, Novocure, and Daiichi Sankyo; and travel, accommodations, or expenses from AstraZeneca, Bristol-Myers Squibb, Boehringer Ingelheim, Roche, Merck, Novartis, prIME Oncology, and Pfizer. Dr. Paz-Ares is a board member of Genomica and has received honoraria from Roche/Genentech, Eli Lilly and Company, Pfizer, Boehringer Ingelheim, Bristol-Myers Squibb, Merck Sharp and Dohme, AstraZeneca, Merck Serono, Pharmamar, Novartis, Celgene, Sysmex, Amgen, and Incyte, as well as travel, accommodations, or expenses from Roche, AstraZeneca, AstraZeneca Spain, Merck Sharp and Dohme, Bristol-Myers Squibb, Eli Lilly and Company, and Pfizer. Dr. Faivre-Finn has received research funding and travel support from Merck, AstraZeneca, and Elekta and travel support only from Pfizer. Dr. Vansteenkiste has received institutional research funding from Merck Sharp and Dohme; advisory fees from Apotex, AstraZeneca, Boehringer Ingelheim, Merck Sharp and Dohme, Novartis, and Roche; and honoraria from AstraZeneca, Bristol-Myers Squibb, Merck Sharp and Dohme, and Roche. Ms. Taboada and Dr. Dennis are full-time employees of AstraZeneca with stock ownership. Ms. Wadsworth was a full-time employee of AstraZeneca when the work was conducted.
The remaining authors declare no conflict of interest.
Figures
References
-
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2018;68:394–424. - PubMed
-
- Walters S, Maringe C, Coleman MP, et al. Lung cancer survival and stage at diagnosis in Australia, Canada, Denmark, Norway, Sweden and the UK: a population-based study, 2004‒2007. Thorax 2013;68:551–564. - PubMed
-
- Bradley JD, Hu C, Komaki RU, et al. Long-term results of RTOG 0617: a randomized phase 3 comparison of standard dose versus high dose conformal chemoradiation therapy ± cetuximab for stage III NSCLC. Int J Radiat Oncol Biol Phys 2017;99(suppl):S105.
