

TAFRO syndrome as a cause of glomerular microangiopathy: a case report and literature review
- PMID: 31623576
- PMCID: PMC6798393
- DOI: 10.1186/s12882-019-1574-9
TAFRO syndrome as a cause of glomerular microangiopathy: a case report and literature review
Abstract
Background: TAFRO syndrome is a systemic inflammatory disorder that manifests as thrombocytopenia (T), anasarca (A), fever (F), reticulin fibrosis (R), and organomegaly (O). Renal dysfunction is frequently complicated with TAFRO syndrome, however, it is challenging to perform kidney biopsy in patients with TAFRO syndrome in the presence of thrombocytopenia. Renal histology in TAFRO syndrome mainly shows membranoproliferative glomerulonephritis (MPGN)-like lesions or thrombotic microangiopathy (TMA)-like glomerulopathy. We review our case and previous reports of TAFRO syndrome with kidney biopsy findings and discuss the renal pathophysiology of TAFRO syndrome.
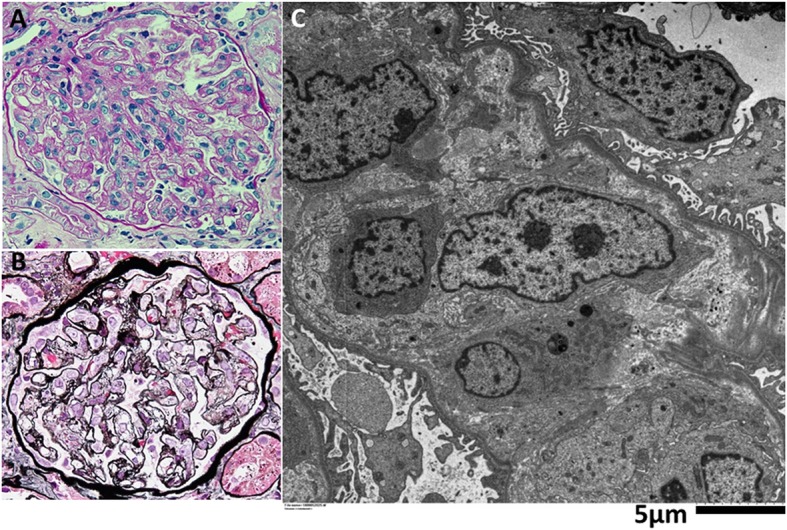
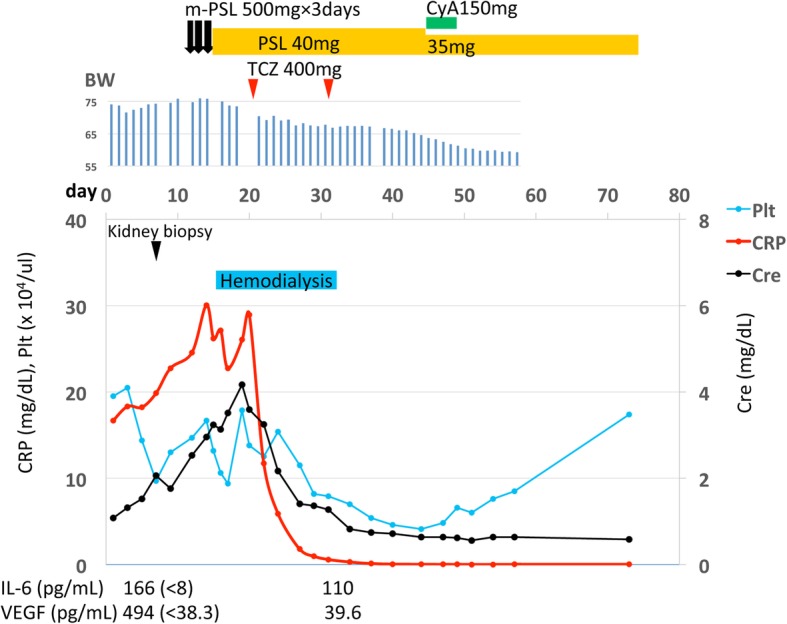
Case presentation: We describe a previously healthy 48- year-old woman with TAFRO syndrome. Kidney biopsy performed before the treatment showed diffuse global endocapillary proliferative changes with endothelial cell swelling, double contours of partial capillary walls, and mesangiolysis, consistent with TMA-like glomerulopathy. Glucocorticoid therapy including steroid pulse was ineffective and she developed anasarca, renal dysfunction and oliguria. Hemodialysis was required. However, the anti-Interleukin (IL)-6 receptor antibody (tocilizumab) therapy was very effective. An increase in urinary volume was achieved about 2 weeks after the tocilizumab therapy and hemodialysis was discontinued. To investigate the renal pathophysiology of TAFRO syndrome, we performed immunohistological staining of vascular endothelial growth factor (VEGF)-A, CD34, and D2-40, in our case and a normal control kidney. Glomerular VEGF-A was especially positive in podocytes both, in the control and in the case, with no significant difference and there was a significant increase of VEGF-A staining area in the cortical peritubular capillaries in the case. Both glomerular and renal cortical CD34 expression were significantly decreased in our case. D2-40 expression in cortex was not significantly different.
Conclusions: We reviewed our case and other 10 previous reports about renal biopsy findings in TAFRO syndrome and found that glomerular microangiopathy was a common finding. IL-6-VEGF-axis-induced glomerular microangiopathy may play a crucial role in developing acute kidney injury in TAFRO syndrome and the anti-IL-6 receptor antibody therapy may be useful for TAFRO syndrome refractory to glucocorticoids. About the pathophysiology of VEGF in TAFRO syndrome, VEGF balance in the glomerulus and perhaps in the peritubular capillary system as well may be critical. Further investigation is needed.
Keywords: Castleman disease; Interleukin (IL)-6; Membranoproliferative glomerulonephritis (MPGN); TAFRO syndrome; Thrombotic microangiopathy (TMA); Tocilizumab; Vascular endothelial growth factor (VEGF).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Kawabata H, Takai K, Kojima M, et al. Castleman-Kojima disease (TAFRO syndrome): a novel systemic inflammatory disease characterized by a constellation of symptoms, namely, thrombocytopenia, ascites (anasarca), microcytic anemia, myelofibrosis, renal dysfunction, and organomegaly: a status report and summary of Fukushima (6 June,2012) and Nagoya meetings (22 September,2012) J Clin Exp Hematop. 2013;53(1):57–61. doi: 10.3960/jslrt.53.57. - DOI - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
