

Early prognostication of neurological outcome by heart rate variability in adult patients with out-of-hospital sudden cardiac arrest
- PMID: 31623658
- PMCID: PMC6798365
- DOI: 10.1186/s13054-019-2603-6
Early prognostication of neurological outcome by heart rate variability in adult patients with out-of-hospital sudden cardiac arrest
Abstract
Background: Most deaths of comatose survivors of out-of-hospital sudden cardiac arrest result from withdrawal of life-sustaining treatment (WLST) decisions based on poor neurological prognostication and the family's intention. Thus, accurate prognostication is crucial to avoid premature WLST decisions. However, targeted temperature management (TTM) with sedation or neuromuscular blockade against shivering significantly affects early prognostication. In this study, we investigated whether heart rate variability (HRV) analysis could prognosticate poor neurological outcome in comatose patients undergoing hypothermic TTM.
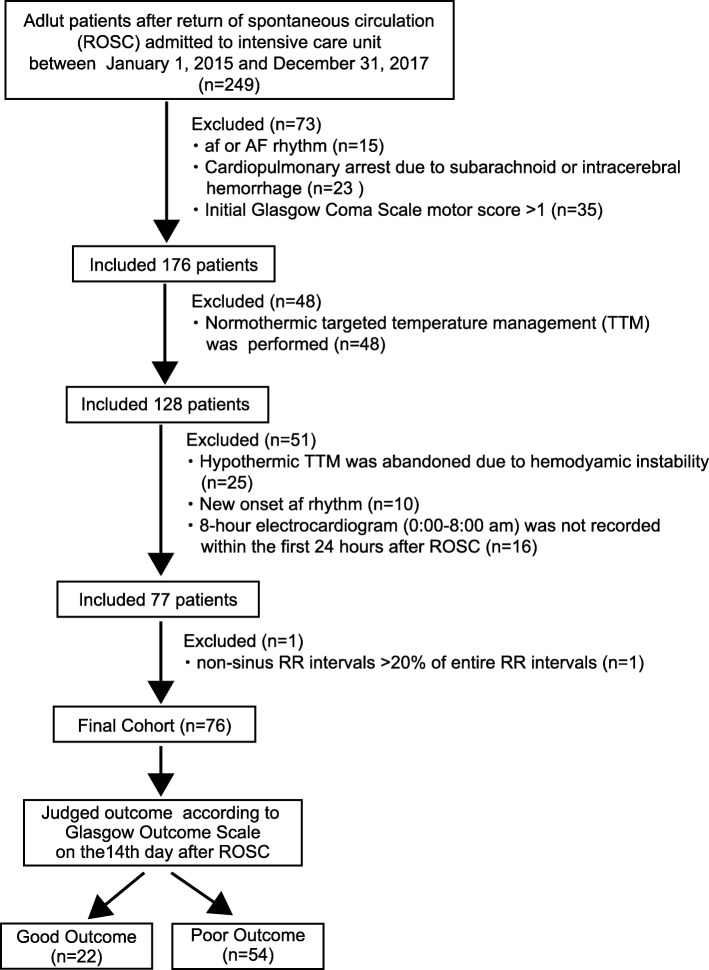
Methods: Between January 2015 and December 2017, adult patients with out-of-hospital sudden cardiac arrest, successfully resuscitated in the emergency department and admitted to the intensive care unit of the Niigata University in Japan, were prospectively included. All patients had an initial Glasgow Coma Scale motor score of 1 and received hypothermic TTM (at 34 °C). Twenty HRV-related variables (deceleration capacity; 4 time-, 3 geometric-, and 7 frequency-domain; and 5 complexity variables) were computed based on RR intervals between 0:00 and 8:00 am within 24 h after return of spontaneous circulation (ROSC). Based on Glasgow Outcome Scale (GOS) at 2 weeks after ROSC, patients were divided into good outcome (GOS 1-2) and poor outcome (GOS 3-5) groups.
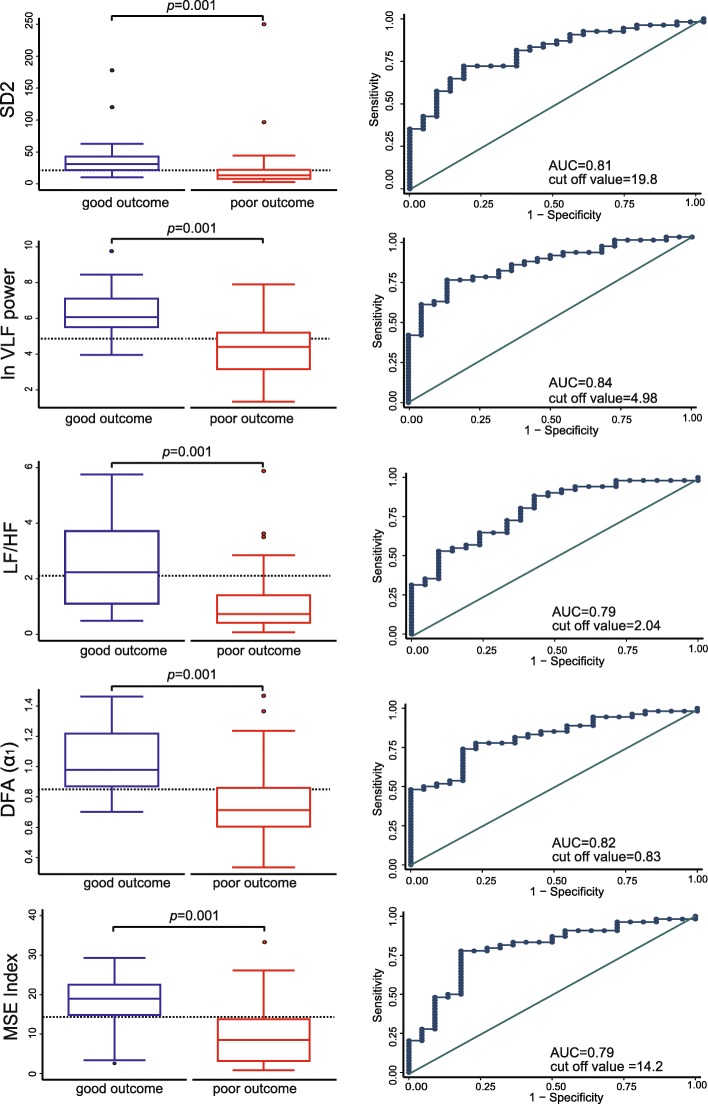
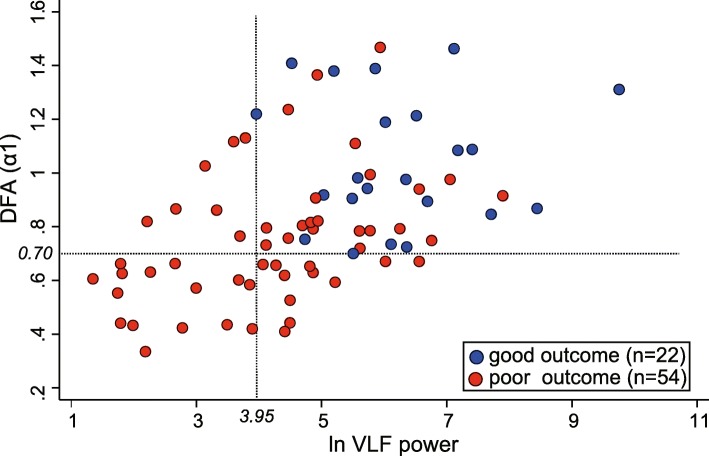
Results: Seventy-six patients were recruited and allocated to the good (n = 22) or poor (n = 54) outcome groups. Of the 20 HRV-related variables, ln very-low frequency (ln VLF) power, detrended fluctuation analysis (DFA) (α1), and multiscale entropy (MSE) index significantly differed between the groups (p = 0.001), with a statistically significant odds ratio (OR) by univariate logistic regression analysis (p = 0.001). Multivariate logistic regression analysis of the 3 variables identified ln VLF power and DFA (α1) as significant predictors for poor outcome (OR = 0.436, p = 0.006 and OR = 0.709, p = 0.024, respectively). The area under the receiver operating characteristic curve for ln VLF power and DFA (α1) in predicting poor outcome was 0.84 and 0.82, respectively. In addition, the minimum value of ln VLF power or DFA (α1) for the good outcome group predicted poor outcome with sensitivity = 61% and specificity = 100%.
Conclusions: The present data indicate that HRV analysis could be useful for prognostication for comatose patients during hypothermic TTM.
Keywords: Glasgow outcome scale; Heart rate variability; Out-of-hospital sudden cardiac arrest; Prognostication; Targeted temperature management.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Callaway CW, Donnino MW, Fink EL, Geocadin RG, Golan E, Kern KB, Leary M, Meurer WJ, Peberdy MA, Thompson TM, Zimmermanet JL. Part 8: post-cardiac arrest care 2015 American Heart Association guidelines update for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2015;132(suppl1):465–482. doi: 10.1161/CIR.0000000000000262. - DOI - PMC - PubMed
-
- Nolan JP, Soar J, Cariou A, Cronberg T, Moulaert VRM, Deakin CD, Bottiger BW, Fribergi H, Sunde K, Sandroni C. European Resuscitation Council and European Society of Intensive Care Medicine Guidelines for post-resuscitation care 2015 section 5 of the European Resuscitation Council guidelines for resuscitation. 2015. Resuscitation. 2015;95:202–222. doi: 10.1016/j.resuscitation.2015.07.018. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
