

The prognostic role of IDH mutations in homogeneously treated patients with anaplastic astrocytomas and glioblastomas
- PMID: 31623667
- PMCID: PMC6798425
- DOI: 10.1186/s40478-019-0817-0
The prognostic role of IDH mutations in homogeneously treated patients with anaplastic astrocytomas and glioblastomas
Abstract
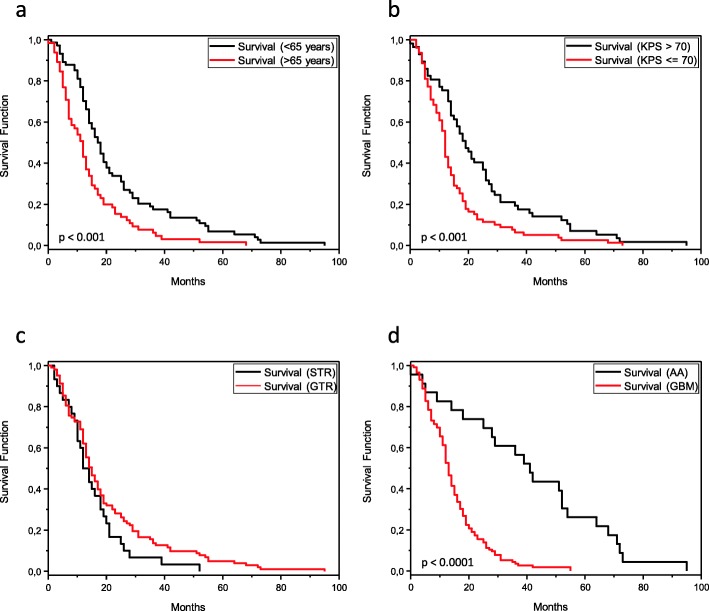
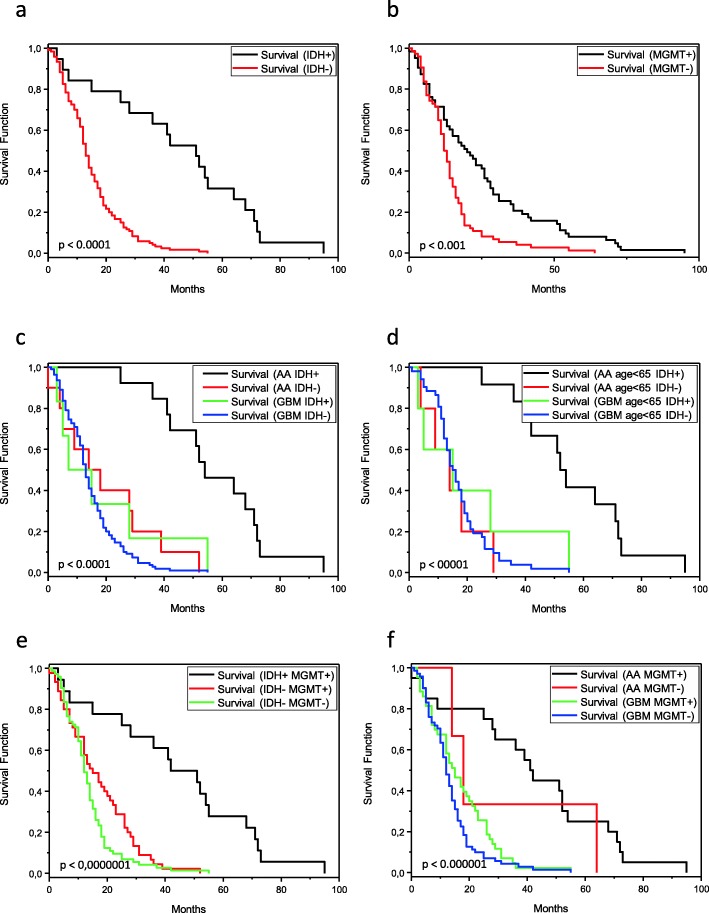
The detection of IDH mutations in patients with diffusely infiltrating malignant astrocytomas resulted in substantial modifications in the concept of WHO classification of these tumors. An important underlying observation was that patients with anaplastic astrocytomas (AA) without IDH mutation had a clinical course similar to that of patients with glioblastomas (GBM). The underlying observations of the German Glioma Network and NOA-04, however, were based on mixed patient cohorts. While most GBM patients received combined radiochemotherapy, patients with AA usually had radiotherapy or chemotherapy only. This intrinsic shortcoming of the study raised the question of whether patients with AA, IDH wildtype, WHO grade III, might have better prognosis if treated with combined radiochemotherapy than patients with GBM receiving the same combination therapy. Thus, the question remains whether the established histopathological grading criteria for malignant astrocytomas in the absence of an IDH mutation are still important if neither vascular proliferation nor necrosis are detectable. All patients in the cohort investigated here with the diagnosis of AA or GBM were subjected to a combined radiochemotherapy according to the Stupp protocol independently of the histopathological diagnosis. Thus, the analysis of these patients allows to clarify whether patients with AA, IDH wildtype, WHO grade III have a prognosis similar to that of GBM, IDH wildtype, WHO grade IV, even under equivalent therapeutic conditions. We determined the IDH1 and IDH2 status by sequencing, the MGMT status by pyrosequencing after bisulfite treatment and the EGFR status of the patients by FISH. In fact, the patients with the histopathological diagnosis of an AA IDH wild-type under similar aggressive therapy showed a comparable and therefore no better prognosis (median overall survival (mOS) 16 months) than patients with a GBM (mOS 13 months). Instead, patients with an AA and an IDH mutation receiving the same therapy had a mOS of 54 months. Thus, it can be concluded that in the absence of an IDH mutation, the established histopathological grading criteria 'necrosis' and 'vascular proliferation' actually lose their prognostic significance. If, on the other hand, patients with malignant astrocytomas and an IDH mutation are examined, there is still a difference between patients with necrosis and/or vascular proliferation and those whose tumors do not show such characteristics. Accordingly, in patients with malignant astrocytomas with IDH mutation it can be concluded that a histological differentiation between AA IDH mutated and GBM IDH mutated remains beneficial from a prognostic perspective.
Keywords: Anaplastic astrocytomas; EGFR; Glioblastomas; Grading; IDH1; IDH2; MGMT; Prognosis.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Kleihues P., Burger P. C., Scheithauer B. W. Histological Typing of Tumours of the Central Nervous System. Berlin, Heidelberg: Springer Berlin Heidelberg; 1993. Histological Classification of Tumours of the Central Nervous System; pp. 5–10.
-
- Kleihues P, Cavenee WK (2000) Pathology and genetics of tumours of the nervous system. IARC press; International Agency for Research on Cancer, City
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
