

Sex-Specific Thresholds of High-Sensitivity Troponin in Patients With Suspected Acute Coronary Syndrome
- PMID: 31623760
- PMCID: PMC6876271
- DOI: 10.1016/j.jacc.2019.07.082
Sex-Specific Thresholds of High-Sensitivity Troponin in Patients With Suspected Acute Coronary Syndrome
Abstract
Background: Major disparities between women and men in the diagnosis, management, and outcomes of acute coronary syndrome are well recognized.
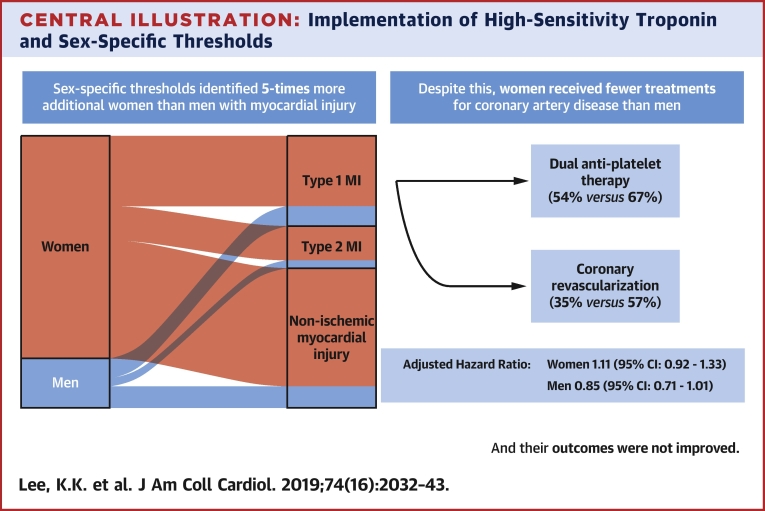
Objectives: The aim of this study was to evaluate the impact of implementing a high-sensitivity cardiac troponin I assay with sex-specific diagnostic thresholds for myocardial infarction in women and men with suspected acute coronary syndrome.
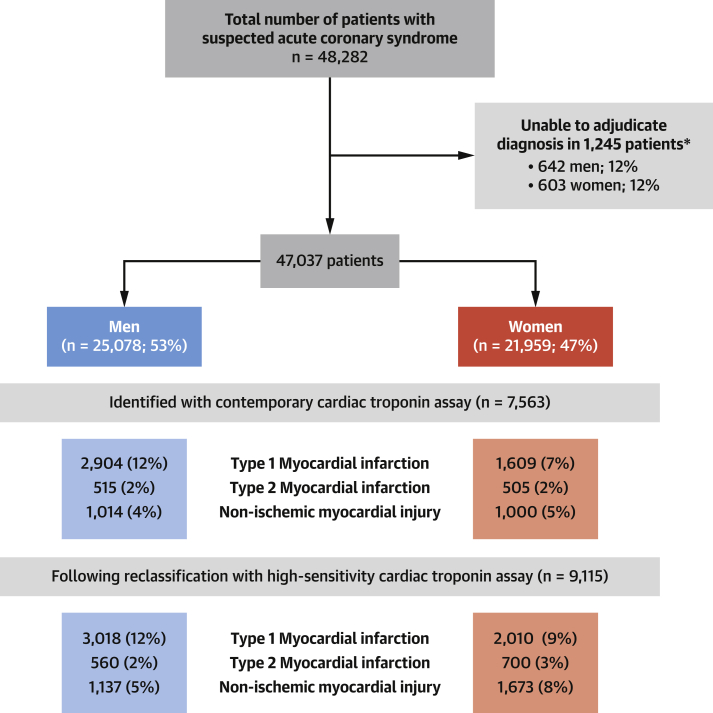
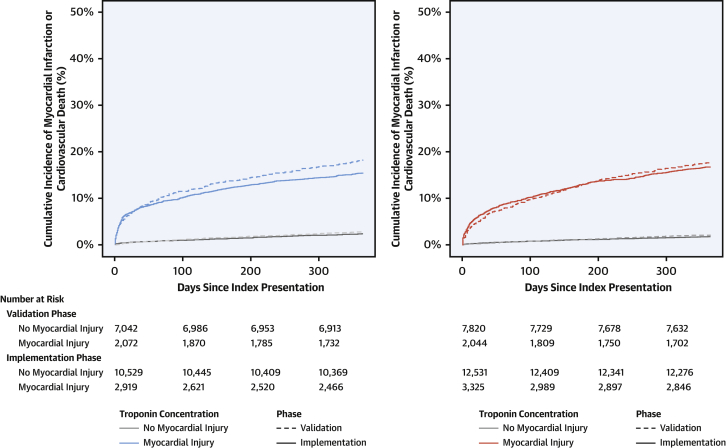
Methods: Consecutive patients with suspected acute coronary syndrome were enrolled in a stepped-wedge, cluster-randomized controlled trial across 10 hospitals. Myocardial injury was defined as high-sensitivity cardiac troponin I concentration >99th centile of 16 ng/l in women and 34 ng/l in men. The primary outcome was recurrent myocardial infarction or cardiovascular death at 1 year.
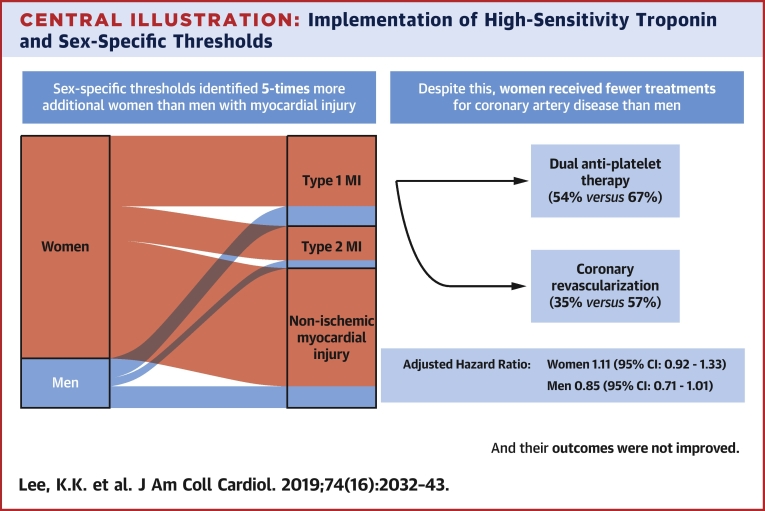
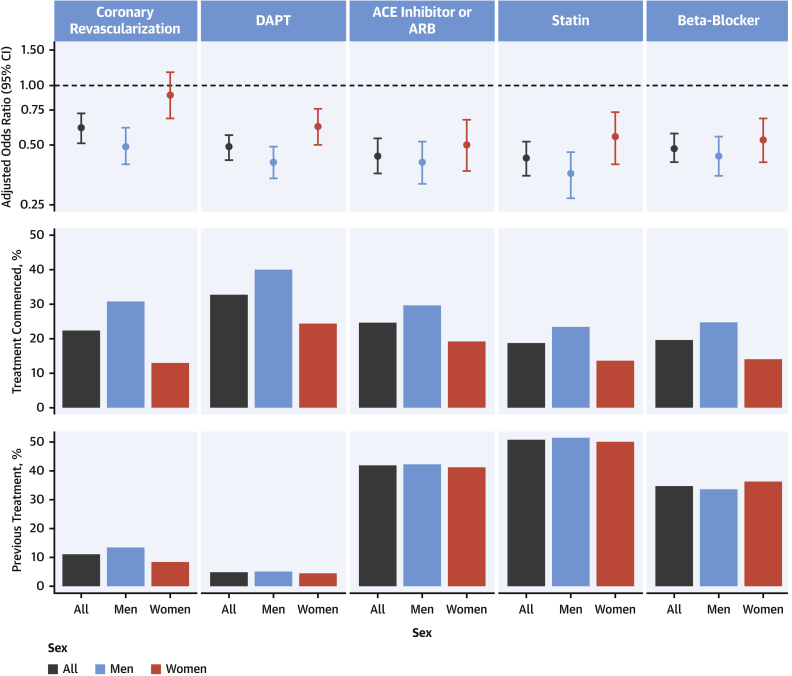
Results: A total of 48,282 patients (47% women) were included. Use of the high-sensitivity cardiac troponin I assay with sex-specific thresholds increased myocardial injury in women by 42% and in men by 6%. Following implementation, women with myocardial injury remained less likely than men to undergo coronary revascularization (15% vs. 34%) and to receive dual antiplatelet (26% vs. 43%), statin (16% vs. 26%), or other preventive therapies (p < 0.001 for all). The primary outcome occurred in 18% (369 of 2,072) and 17% (488 of 2,919) of women with myocardial injury before and after implementation, respectively (adjusted hazard ratio: 1.11; 95% confidence interval: 0.92 to 1.33), compared with 18% (370 of 2,044) and 15% (513 of 3,325) of men (adjusted hazard ratio: 0.85; 95% confidence interval: 0.71 to 1.01).
Conclusions: Use of sex-specific thresholds identified 5 times more additional women than men with myocardial injury. Despite this increase, women received approximately one-half the number of treatments for coronary artery disease as men, and outcomes were not improved. (High-Sensitivity Troponin in the Evaluation of Patients With Acute Coronary Syndrome [High-STEACS]; NCT01852123).
Keywords: acute coronary syndrome; high-sensitivity cardiac troponin; myocardial infarction; sex-specific threshold.
Copyright © 2019. Published by Elsevier Inc.
Figures
Comment in
-
It Will Take More Than Better Diagnostics to Improve the Care of Women With ACS.J Am Coll Cardiol. 2019 Oct 22;74(16):2044-2046. doi: 10.1016/j.jacc.2019.08.1012. J Am Coll Cardiol. 2019. PMID: 31623761 No abstract available.
References
-
- Wenger N.K. Women and coronary heart disease: a century after Herrick: understudied, underdiagnosed, and undertreated. Circulation. 2012;126:604–611. - PubMed
-
- Thygesen K., Alpert J.S., Jaffe A.S. Fourth universal definition of myocardial infarction (2018) J Am Coll Cardiol. 2018;72:2231–2264. - PubMed
-
- Mehta L.S., Beckie T.M., DeVon H.A. Acute myocardial infarction in women: a scientific statement from the American Heart Association. Circulation. 2016;133:916–947. - PubMed
-
- Apple F.S., Ler R., Murakami M.M. Determination of 19 cardiac troponin I and T assay 99th percentile values from a common presumably healthy population. Clin Chem. 2012;58:1574–1581. - PubMed
-
- Apple F.S., Collinson P.O., for the IFCC Task Force on Clinical Applications of Cardiac Biomarkers Analytical characteristics of high-sensitivity cardiac troponin assays. Clin Chem. 2012;58:54–61. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
