

Guiding Therapy by Coronary CT Angiography Improves Outcomes in Patients With Stable Chest Pain
- PMID: 31623764
- PMCID: PMC6899446
- DOI: 10.1016/j.jacc.2019.07.085
Guiding Therapy by Coronary CT Angiography Improves Outcomes in Patients With Stable Chest Pain
Abstract
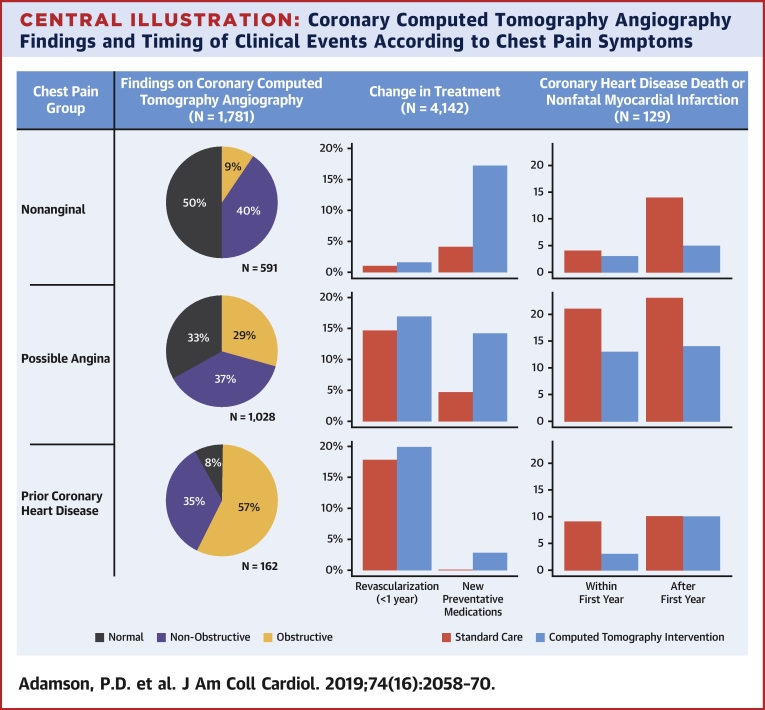
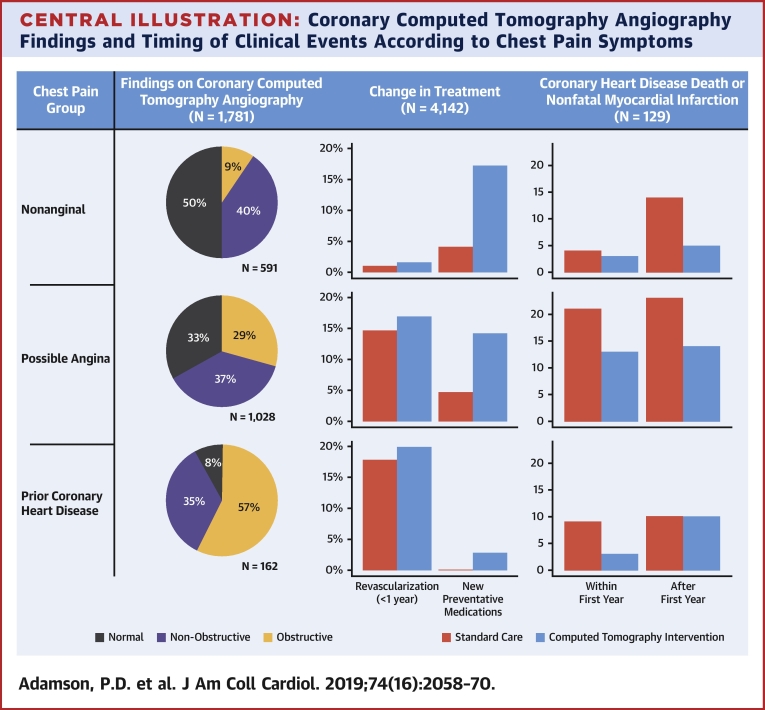
Background: Within the SCOT-HEART (Scottish COmputed Tomography of the HEART Trial) trial of patients with stable chest pain, the use of coronary computed tomography angiography (CTA) reduced the rate of death from coronary heart disease or nonfatal myocardial infarction (primary endpoint).
Objectives: This study sought to assess the consistency and mechanisms of the 5-year reduction in this endpoint.
Methods: In this open-label trial, 4,146 participants were randomized to standard care alone or standard care plus coronary CTA. This study explored the primary endpoint by symptoms, diagnosis, coronary revascularizations, and preventative therapies.
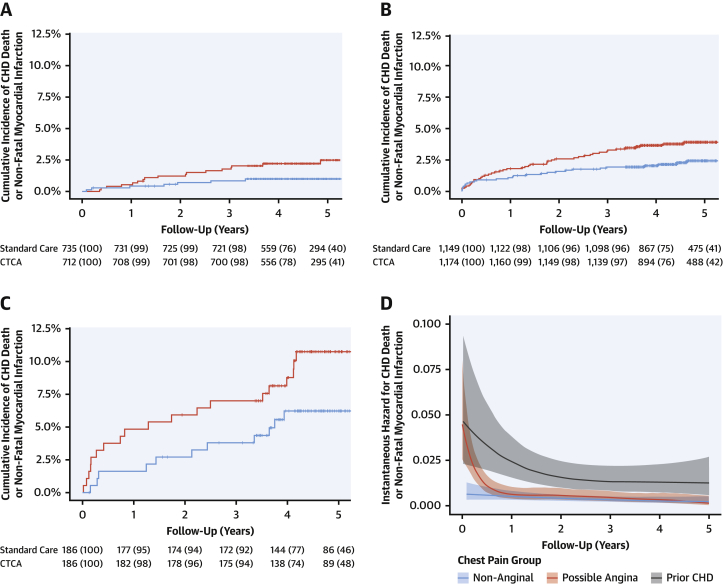
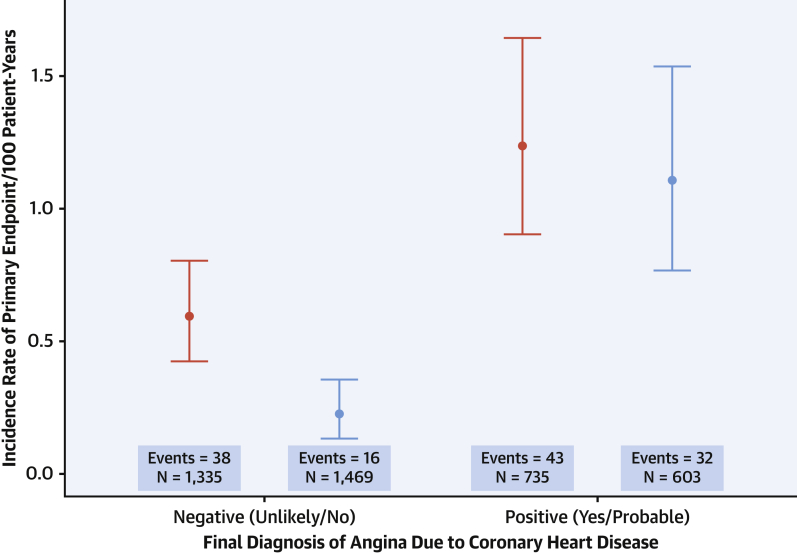
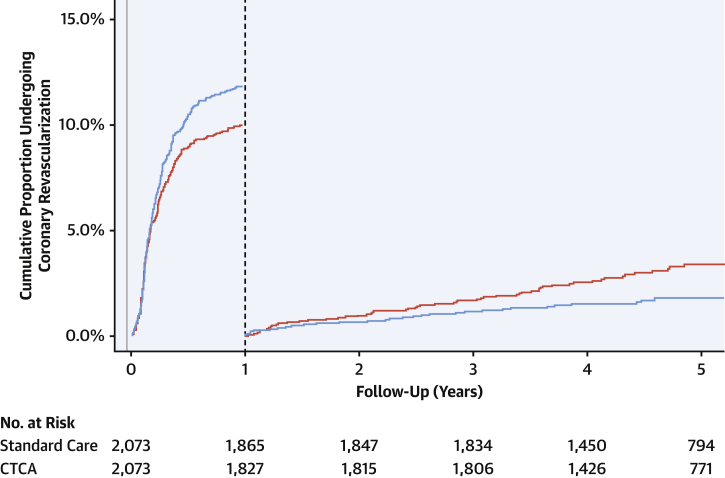
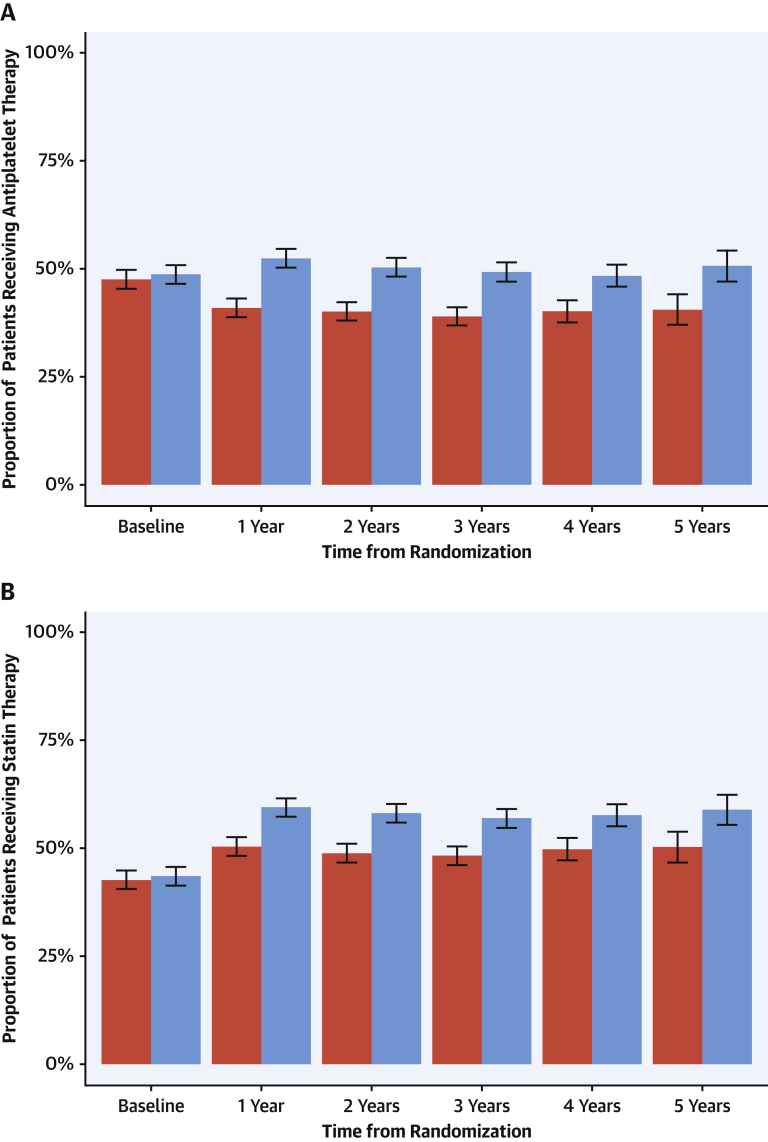
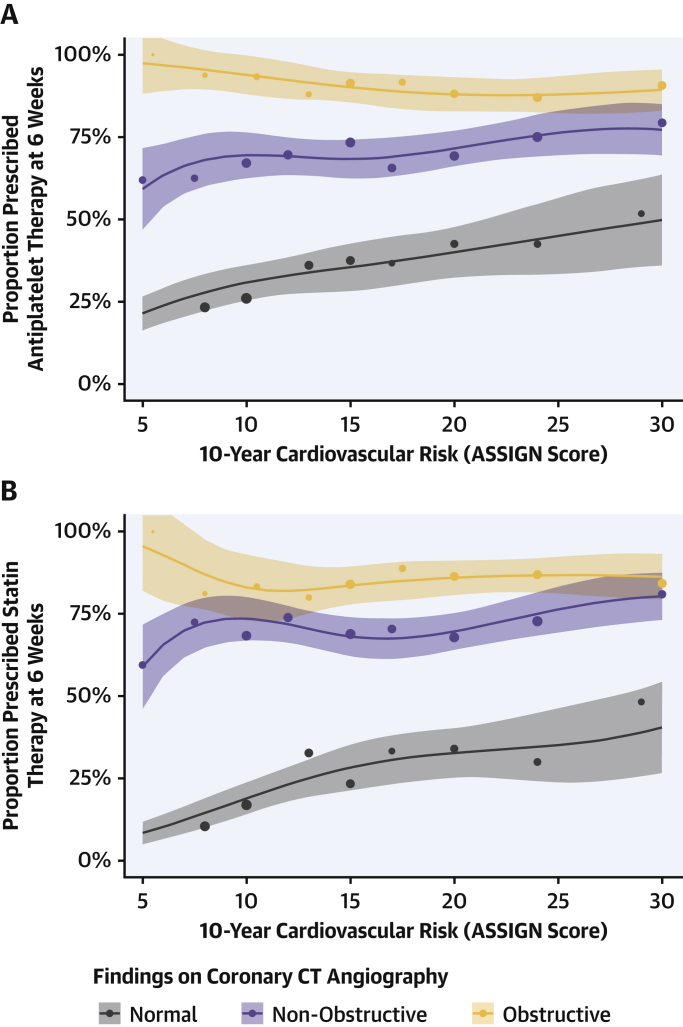
Results: Event reductions were consistent across symptom and risk categories (p = NS for interactions). In patients who were not diagnosed with angina due to coronary heart disease, coronary CTA was associated with a lower primary endpoint incidence rate (0.23; 95% confidence interval [CI]: 0.13 to 0.35 vs. 0.59; 95% CI: 0.42 to 0.80 per 100 patient-years; p < 0.001). In those who had undergone coronary CTA, rates of coronary revascularization were higher in the first year (hazard ratio [HR]: 1.21; 95% CI: 1.01 to 1.46; p = 0.042) but lower beyond 1 year (HR: 0.59; 95% CI: 0.38 to 0.90; p = 0.015). Patients assigned to coronary CTA had higher rates of preventative therapies throughout follow-up (p < 0.001 for all), with rates highest in those with CT-defined coronary artery disease. Modeling studies demonstrated the plausibility of the observed effect size.
Conclusions: The beneficial effect of coronary CTA on outcomes is consistent across subgroups with plausible underlying mechanisms. Coronary CTA improves coronary heart disease outcomes by enabling better targeting of preventative treatments to those with coronary artery disease. (Scottish COmputed Tomography of the HEART Trial [SCOT-HEART]; NCT01149590).
Keywords: angina pectoris; computed tomography; coronary heart disease.
Copyright © 2019 The Authors. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Time for a Change or Just a Reason to Question Further?J Am Coll Cardiol. 2019 Oct 22;74(16):2071-2073. doi: 10.1016/j.jacc.2019.08.1014. J Am Coll Cardiol. 2019. PMID: 31623765 No abstract available.
References
-
- Montalescot G., Sechtem U., Achenbach S., for the European Society of Cardiology Task Force 2013 ESC guidelines on the management of stable coronary artery disease: the Task Force on the management of stable coronary artery disease of the European Society of Cardiology. Eur Heart J. 2013;34:2949–3003. - PubMed
-
- Miller J.M., Rochitte C.E., Dewey M. Diagnostic performance of coronary angiography by 64-row CT. N Engl J Med. 2008;359:2324–2336. - PubMed
-
- The SCOT-HEART Investigators CT coronary angiography in patients with suspected angina due to coronary heart disease (SCOT-HEART): an open-label, parallel-group, multicentre trial. Lancet. 2015;385:2383–2391. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
