

Coadministered cannabidiol and clobazam: Preclinical evidence for both pharmacodynamic and pharmacokinetic interactions
- PMID: 31625159
- PMCID: PMC6900043
- DOI: 10.1111/epi.16355
Coadministered cannabidiol and clobazam: Preclinical evidence for both pharmacodynamic and pharmacokinetic interactions
Abstract
Objective: Cannabidiol (CBD) has been approved by the US Food and Drug Administration (FDA) to treat intractable childhood epilepsies, such as Dravet syndrome and Lennox-Gastaut syndrome. However, the intrinsic anticonvulsant activity of CBD has been questioned due to a pharmacokinetic interaction between CBD and a first-line medication, clobazam. This recognized interaction has led to speculation that the anticonvulsant efficacy of CBD may simply reflect CBD augmenting clobazam exposure. The present study aimed to address the nature of the interaction between CBD and clobazam.
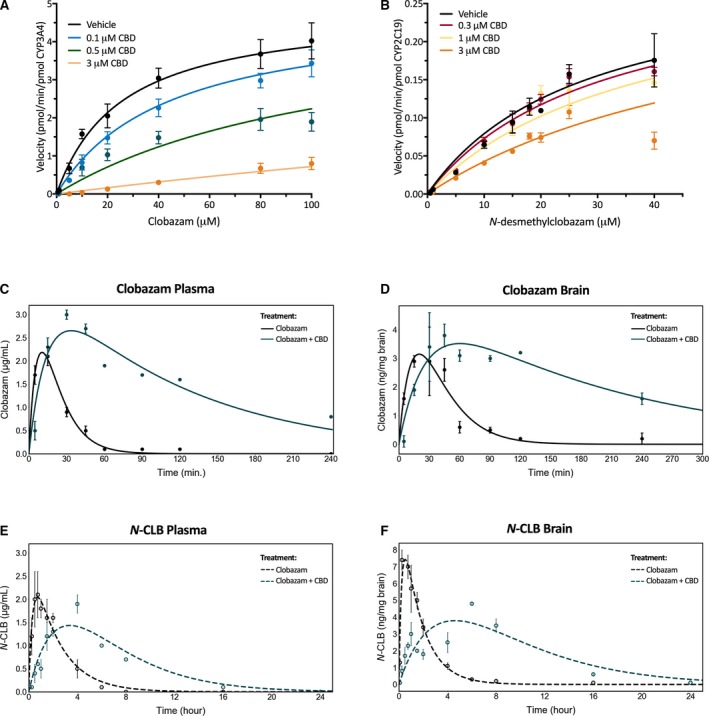
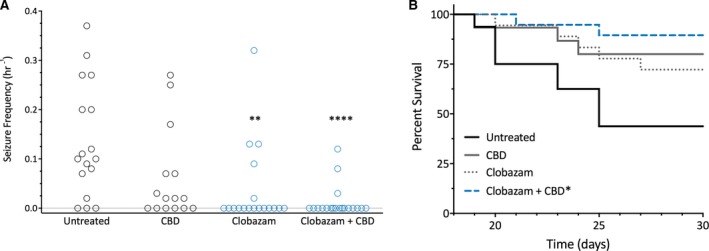
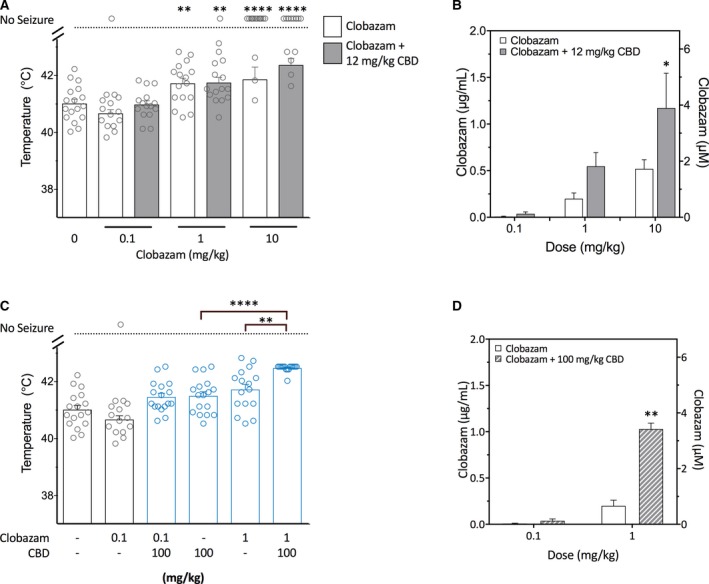
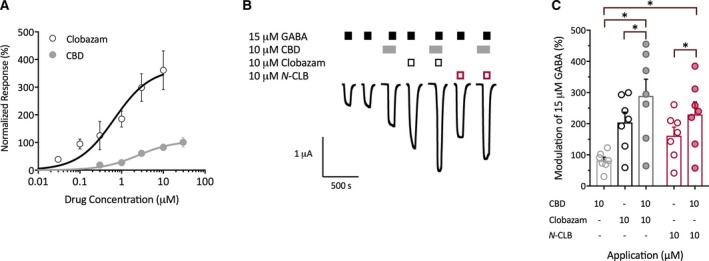
Methods: We examined whether CBD inhibits human CYP3A4 and CYP2C19 mediated metabolism of clobazam and N-desmethylclobazam (N-CLB), respectively, and performed studies assessing the effects of CBD on brain and plasma pharmacokinetics of clobazam in mice. We then used the Scn1a+/- mouse model of Dravet syndrome to examine how CBD and clobazam interact. We compared anticonvulsant effects of CBD-clobazam combination therapy to monotherapy against thermally-induced seizures, spontaneous seizures and mortality in Scn1a+/- mice. In addition, we used Xenopus oocytes expressing γ-aminobutyric acid (GABA)A receptors to investigate the activity of GABAA receptors when treated with CBD and clobazam together.
Results: CBD potently inhibited CYP3A4 mediated metabolism of clobazam and CYP2C19 mediated metabolism of N-CLB. Combination CBD-clobazam treatment resulted in greater anticonvulsant efficacy in Scn1a+/- mice, but only when an anticonvulsant dose of CBD was used. It is important to note that a sub-anticonvulsant dose of CBD did not promote greater anticonvulsant effects despite increasing plasma clobazam concentrations. In addition, we delineated a novel pharmacodynamic mechanism where CBD and clobazam together enhanced inhibitory GABAA receptor activation.
Significance: Our study highlights the involvement of both pharmacodynamic and pharmacokinetic interactions between CBD and clobazam that may contribute to its efficacy in Dravet syndrome.
Keywords: Dravet syndrome; cannabidiol; cannabis; clobazam; epilepsy.
© 2019 The Authors. Epilepsia published by Wiley Periodicals, Inc. on behalf of International League Against Epilepsy.
Conflict of interest statement
Associate Professor Jonathon Arnold is Deputy Academic Director of the Lambert Initiative. He has served as an expert witness in various medicolegal cases involving cannabis and recently served as a temporary advisor to the World Health Organization (WHO) on their review of cannabis and the cannabinoids. His research is also funded by the NHMRC. Professor Iain McGregor is academic director of the Lambert Initiative and an NHMRC Principal Research Fellow, and he receives research funding from the Australian Research Council and NHMRC. He is involved in an NHMRC‐funded clinical trial using the cannabis extract, nabiximols (Sativex). He has served as an expert witness in various medicolegal cases involving cannabis and cannabinoids. A/Prof Arnold, Prof McGregor and Dr Lyndsey Anderson hold a patent on a novel anticonvulsant therapy for epilepsy. The remaining authors have no conflicts of interest. We confirm that we have read the Journal's position on issues involved in ethical publication and affirm that this report is consistent with those guidelines.
Figures
Comment in
-
Commentary on: Coadministered cannabidiol and clobazam: Preclinical evidence for both pharmacodynamic and pharmacokinetic interactions.Epilepsia. 2020 Oct;61(10):2063-2064. doi: 10.1111/epi.16660. Epub 2020 Aug 17. Epilepsia. 2020. PMID: 33460074 No abstract available.
References
-
- Devinsky O, Cross JH, Laux L, Marsh E, Miller I, Nabbout R, et al. Trial of cannabidiol for drug resistant seizure in the Dravet Syndrome. N Engl J Med. 2017;376:2011–20. - PubMed
-
- Thiele EA, Marsh ED, French JA, Mazurkiewicz‐Beldzinska M, Benbadis SR, Joshi C, et al. Cannabidiol in patients with seizures associated with Lennox‐Gastaut syndrome (GWPCARE4): a randomised, double‐blind, placebo‐controlled phase 3 trial. Lancet. 2018;391:1085–96. - PubMed
-
- Greenwood SM, VanLandingham KE, Cross JH, Villanueva V, Wirrell EC, Privitera M, et al. Effect of cannabidiol on drop seizures in the Lennox–Gastaut Syndrome. N Engl J Med. 2018;378:1888–97. - PubMed
-
- Dravet C. The core Dravet syndrome phenotype. Epilepsia. 2011;52:3–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
