

Immune responses in the human female reproductive tract
- PMID: 31630394
- PMCID: PMC7218661
- DOI: 10.1111/imm.13136
Immune responses in the human female reproductive tract
Abstract
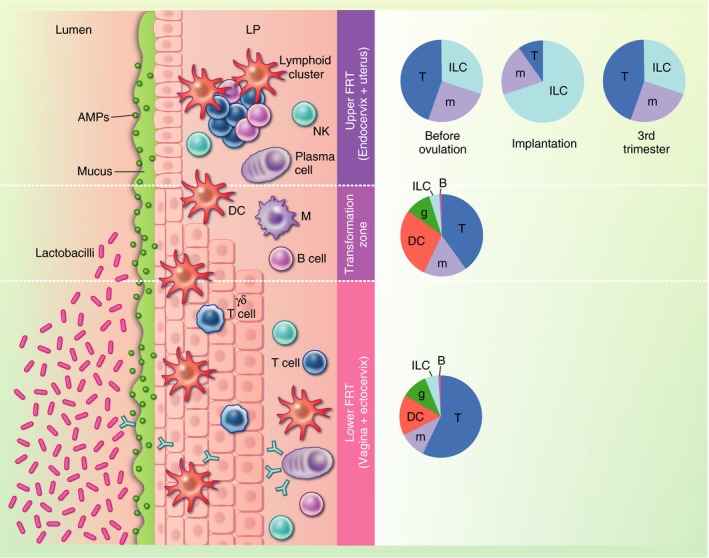
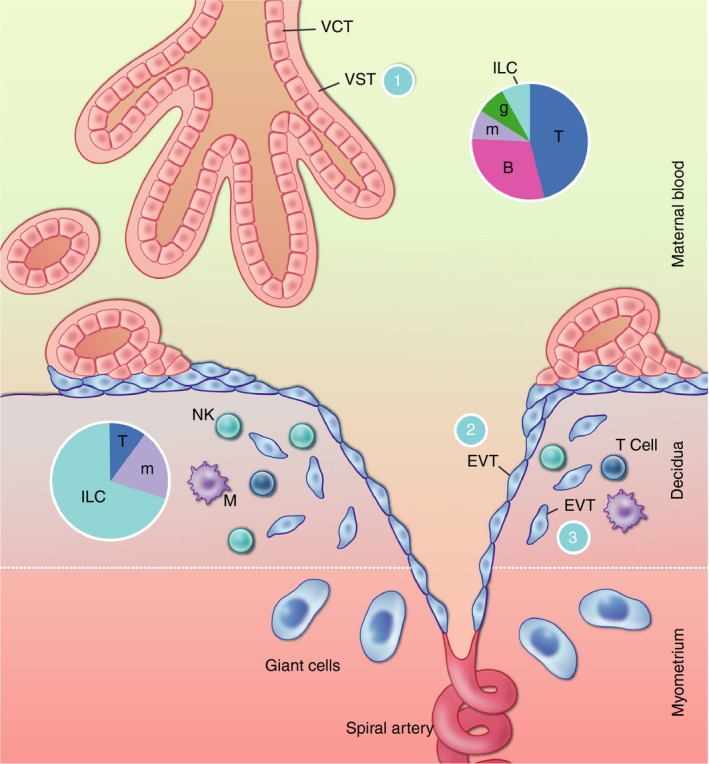
Mucosal surfaces are key interfaces between the host and its environment, but also constitute ports of entry for numerous pathogens. The gut and lung mucosae act as points of nutrient and gas exchange, respectively, but the physiological purpose of the female reproductive tract (FRT) is to allow implantation and development of the fetus. Our understanding of immune responses in the FRT has traditionally lagged behind our grasp of the situation at other mucosal sites, but recently reproductive immunologists have begun to make rapid progress in this challenging area. Here, we review current knowledge of immune responses in the human FRT and their heterogeneity within and between compartments. In the commensal-rich vagina, the immune system must allow the growth of beneficial microbes, whereas the key challenge in the uterus is allowing the growth of the semi-allogeneic fetus. In both compartments, these objectives must be balanced with the need to eliminate pathogens. Our developing understanding of immune responses in the FRT will help us develop interventions to prevent the spread of sexually transmitted diseases and to improve outcomes of pregnancy for mothers and babies.
Keywords: ILC; T-cells; macrophages; mucosa; uterus.
© 2019 John Wiley & Sons Ltd.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
