

3D Whole-heart free-breathing qBOOST-T2 mapping
- PMID: 31631378
- PMCID: PMC7004111
- DOI: 10.1002/mrm.28039
3D Whole-heart free-breathing qBOOST-T2 mapping
Abstract
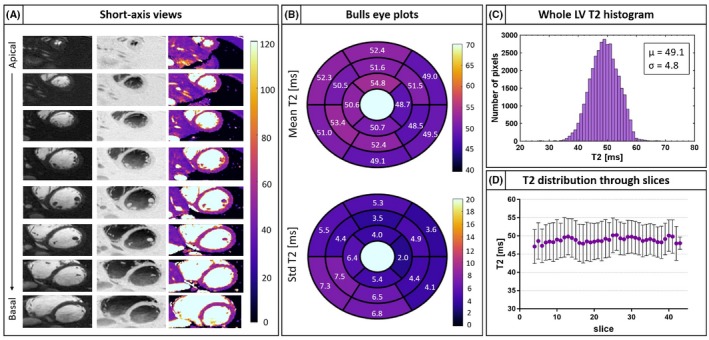
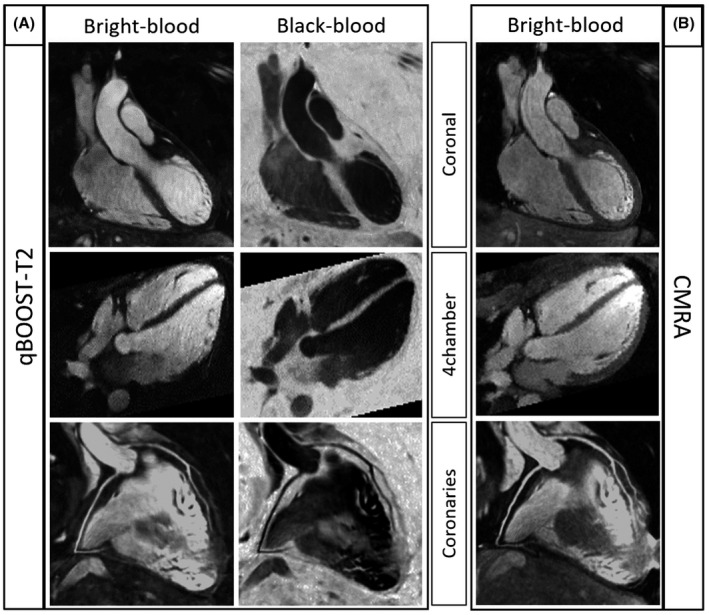
Purpose: To develop an accelerated motion corrected 3D whole-heart imaging approach (qBOOST-T2) for simultaneous high-resolution bright- and black-blood cardiac MR imaging and quantitative myocardial T2 characterization.
Methods: Three undersampled interleaved balanced steady-state free precession cardiac MR volumes were acquired with a variable density Cartesian trajectory and different magnetization preparations: (1) T2-prepared inversion recovery (T2prep-IR), (2) T2-preparation, and (3) no preparation. Image navigators were acquired prior the acquisition to correct for 2D translational respiratory motion. Each 3D volume was reconstructed with a low-rank patch-based reconstruction. The T2prep-IR volume provides bright-blood anatomy visualization, the black-blood volume is obtained by means of phase sensitive reconstruction between first and third datasets, and T2 maps are generated by matching the signal evolution to a simulated dictionary. The proposed sequence has been evaluated in simulations, phantom experiments, 11 healthy subjects and compared with 3D bright-blood cardiac MR and standard 2D breath-hold balanced steady-state free precession T2 mapping. The feasibility of the proposed approach was tested on 4 patients with suspected cardiovascular disease.
Results: High linear correlation (y = 1.09 × -0.83, R2 = 0.99) was found between the proposed qBOOST-T2 and T2 spin echo measurements in phantom experiment. Good image quality was observed in vivo with the proposed 4x undersampled qBOOST-T2. Mean T2 values of 53.1 ± 2.1 ms and 55.8 ± 2.7 ms were measured in vivo for 2D balanced steady-state free precession T2 mapping and qBOOST-T2, respectively, with linear correlation of y = 1.02x+1.46 (R2 = 0.61) and T2 bias = 2.7 ms.
Conclusion: The proposed qBOOST-T2 sequence allows the acquisition of 3D high-resolution co-registered bright- and black-blood volumes and T2 maps in a single scan of ~11 min, showing promising results in terms of T2 quantification.
Keywords: 3D whole-heart; T2 mapping; black-blood imaging; bright-blood cardiac anatomy; respiratory motion correction.
© 2019 The Authors. Magnetic Resonance in Medicine published by Wiley Periodicals, Inc. on behalf of International Society for Magnetic Resonance in Medicine.
Figures








References
-
- Marcotte F, Poirier N, Pressacco J, et al. Evaluation of adult congenital heart disease by cardiac magnetic resonance imaging. Congenit Heart Dis. 2009;4:216–230. - PubMed
-
- Kim WY, Danias PG, Stuber M, et al. Coronary magnetic resonance angiography for the detection of coronary stenoses. N Engl J Med. 2001;345:1863–1869. - PubMed
-
- Jansen C, Perera D, Makowski MR, et al. Detection of intracoronary thrombus by magnetic resonance imaging in patients with acute myocardial infarction. Circulation. 2011;124:416 LP‐424. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
