

Impaired cognition predicts the risk of hospitalization and death in cirrhosis
- PMID: 31631586
- PMCID: PMC6856598
- DOI: 10.1002/acn3.50924
Impaired cognition predicts the risk of hospitalization and death in cirrhosis
Abstract
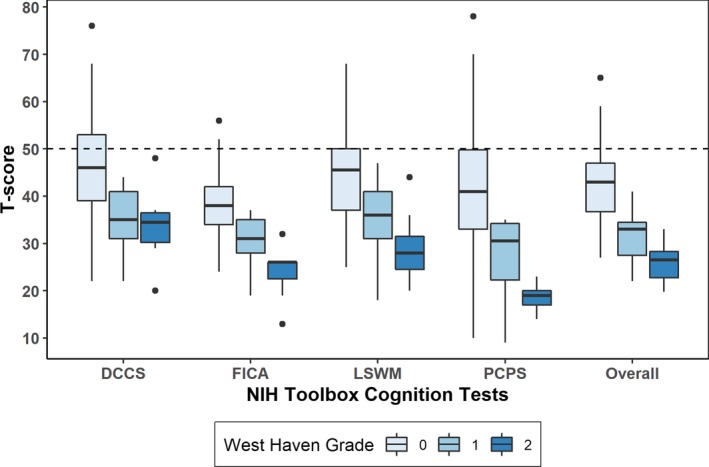
Objective: Cognitive impairment, detected in up to 80% of patients with liver cirrhosis, is associated with negative health outcomes but is underdiagnosed in the clinical setting due to the lack of practical testing method. This single-center prospective observational study aimed to test the feasibility and prognostic utility of in-clinic cognitive assessment of patients with liver cirrhosis using the NIH Toolbox cognition battery (NIHTB).
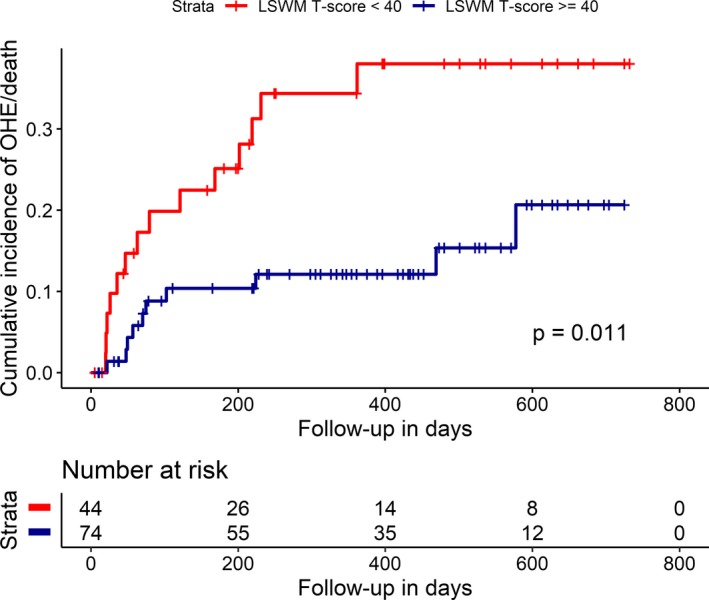
Methods: Patients recruited from a hepatology/transplant clinic underwent cognitive assessments using West-Haven Grade (WHG) and NIHTB between November 2016 and August 2018 and were prospectively followed until December 2018. The primary outcome was a composite end point of hospitalization related to overt hepatic encephalopathy (OHE) and all-cause mortality during follow-up, evaluated by a Cox proportional hazards regression model that adjusted for a priori covariates (age and MELD-Na).
Results: Among 127 patients (median age 60 years, 48 [38%] women) assessed, cognitive performance was significantly impaired in 82 [78%] patients with WHG 0 and 22 [100%] patients with WHG 1 and 2. Over a median of 347 days follow-up, 18 OHE and 8 deaths were observed. Lower cognitive performance was associated with an increased risk of OHE/death adjusting for age and MELD-Na. Subclinical cognitive impairment detected by NIH Toolbox in WHG 0 patients was significantly associated with greater mortality. Median time to complete the two prognostically informative NIH Toolbox tests was 9.4 min.
Interpretation: NIH Toolbox may enable a rapid cognitive screening in the outpatient setting and identify patients at high risk for death and hospitalization for severe encephalopathy.
© 2019 The Authors. Annals of Clinical and Translational Neurology published by Wiley Periodicals, Inc on behalf of American Neurological Association.
Conflict of interest statement
The authors of this manuscript declare no conflicts of interest.
Figures
References
-
- Martin P, DiMartini A, Feng S, et al. Evaluation for liver transplantation in adults: 2013 practice guideline by the American Association for the Study of Liver Diseases and the American Society of. Transplantation 2014;59:1144–65. - PubMed
-
- Bajaj JS, O’Leary JG, Tandon P, et al. Hepatic encephalopathy is associated with mortality in patients with cirrhosis independent of other extrahepatic organ failures. Clin Gastroenterol Hepatol 2017;15:565–574.e4. - PubMed
-
- Neff G. Pharmacoeconomics of hepatic encephalopathy. Pharmacotherapy. 2010;30(5, part 2):28S–32S. - PubMed
-
- Bajaj JS, Wade JB, Sanyal AJ. Spectrum of neurocognitive impairment in cirrhosis: Implications for the assessment of hepatic encephalopathy. Hepatology 2009;50:2014–2021. - PubMed
-
- Das A, Dhiman RK, Saraswat VA, et al. Prevalence and natural history of subclinical hepatic encephalopathy in cirrhosis. J Gastroenterol Hepatol. 2001;16:531–535. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
