

Bracing In The Treatment Of Adolescent Idiopathic Scoliosis: Evidence To Date
- PMID: 31632169
- PMCID: PMC6790111
- DOI: 10.2147/AHMT.S190565
Bracing In The Treatment Of Adolescent Idiopathic Scoliosis: Evidence To Date
Abstract
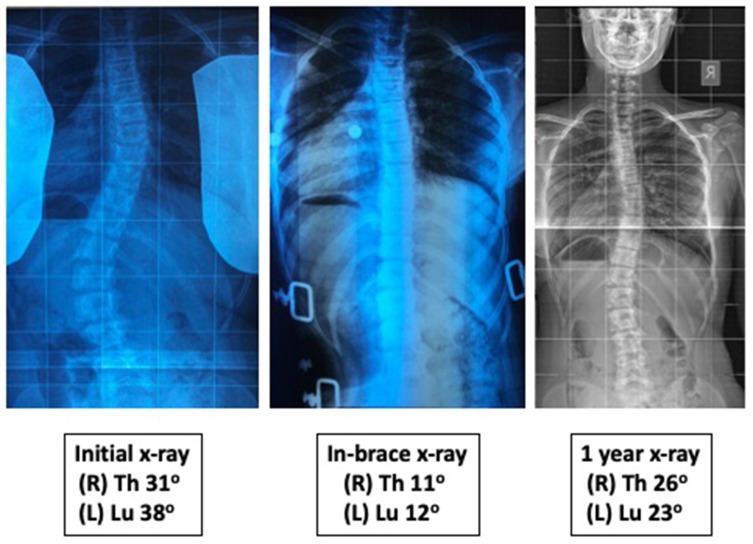
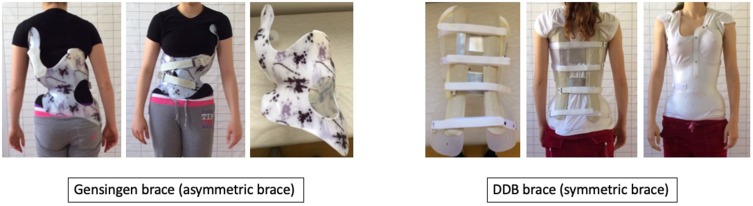
Brace effectiveness for adolescent idiopathic scoliosis was controversial until recent studies provided high quality of evidence that bracing can decrease likelihood of progression and need for operative treatment. Very low evidence exists regarding bracing over 40ο and adult degenerative scoliosis. Initial in-brace correction and compliance seem to be the most important predictive factors for successful treatment outcome. However, the amount of correction and adherence to wearing hours have not been established yet. Moderate evidence suggests that thoracic and double curves, and curves over 30ο at an early growth stage have more risk for failure. High and low body mass index scores are also associated with low successful rates. CAD/CAM braces have shown better initial correction and are more comfortable than conventional plaster cast braces. For a curve at high risk of progression, rigid and day-time braces are significantly more effective than soft or night-time braces. No safe conclusion on effectiveness can be drawn while comparing symmetrical and asymmetrical brace designs. The addition of physiotherapeutic scoliosis-specific exercises in brace treatment can provide better outcomes and is recommended, when possible. Despite the growing evidence for brace effectiveness, there is still an imperative need for future high methodological quality studies to be conducted.
Keywords: brace; evidence; non-operative treatment; orthosis; scoliosis.
© 2019 Karavidas.
Conflict of interest statement
The author reports no conflicts of interest in this work.
Figures


References
-
- Negrini S, Hresko T, O’Brien J, Price N; SOSORT Boards and SRS Non-Operative Committee. Recommendations for research studies on treatment of idiopathic scoliosis: consensus 2014 between SOSORT and SRS non-operative management committee. Scoliosis. 2015;10:8. doi:10.1186/s13013-014-0025-4 - DOI - PMC - PubMed
-
- Lonstein JE, Carlson JM. The prediction of curve progression in untreated idiopathic scoliosis during growth. J Bone Joint Surg Am. 1984;66(7):1061–1071. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
