

Management of irritable bowel syndrome with diarrhea: a review of nonpharmacological and pharmacological interventions
- PMID: 31632456
- PMCID: PMC6778998
- DOI: 10.1177/1756284819878950
Management of irritable bowel syndrome with diarrhea: a review of nonpharmacological and pharmacological interventions
Abstract
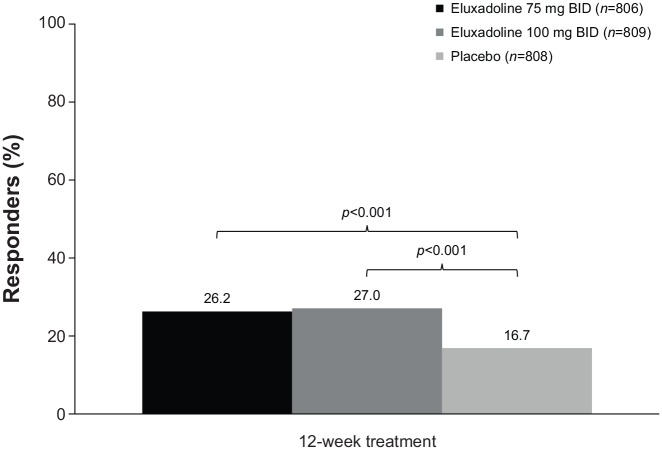
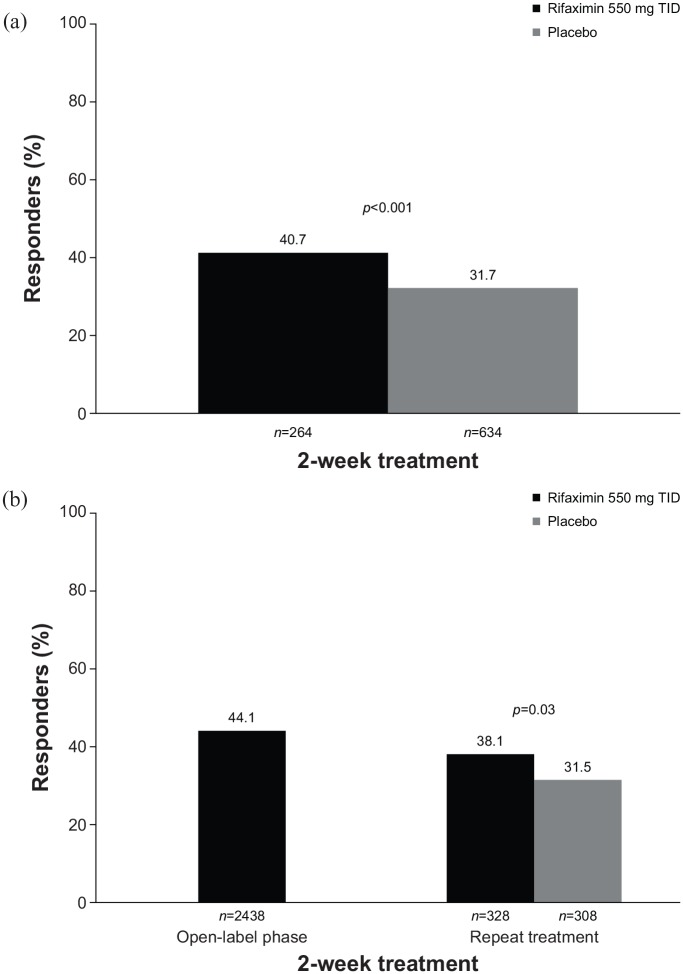
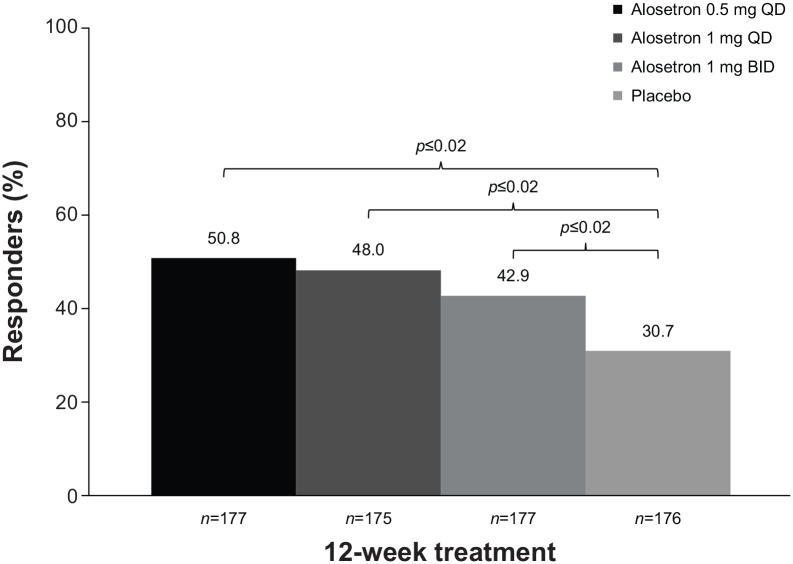
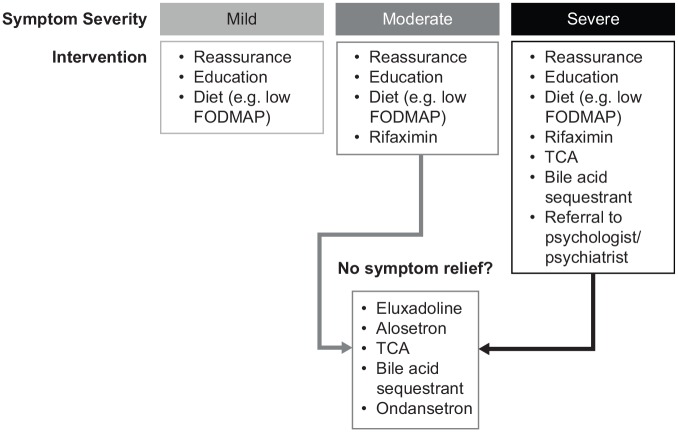
Irritable bowel syndrome (IBS) is a common gastrointestinal (GI) condition involving numerous potential causative factors (e.g. alterations in gut microbiota, motility, brain-gut axis). Several interventions are available for the management of patients with IBS, but no universal management algorithm currently exists. The aim of this article is to review interventions that may be considered in the management of patients with IBS with diarrhea (IBS-D). Nonpharmacological interventions include dietary and lifestyle modification, which are generally used as first-line therapy. Probiotics have demonstrated efficacy and safety in patients with IBS, but studies are inconsistent in strains examined, dosing, and treatment duration. Psychological therapies (e.g. cognitive behavioral therapy, hypnotherapy) also may improve IBS symptoms. Pharmacological interventions for the management of IBS-D include the US Food and Drug Administration-approved agents eluxadoline, rifaximin, and alosetron, as well as loperamide, smooth muscle antispasmodics, bile acid sequestrants, and antidepressants (i.e. tricyclic antidepressants, selective serotonin reuptake inhibitors). Eluxadoline and rifaximin have been shown to improve abdominal pain and stool consistency in patients with IBS-D. In addition, data indicate that alosetron improves IBS symptoms; however, it is approved only for women with severe IBS-D. Of the three approved agents, rifaximin has the most favorable safety profile. The risk-benefit ratio is an important consideration with every medication, but is especially important in the treatment of functional GI disorders such as IBS-D. Thus, the most troublesome symptoms, quality of life, symptom intensity, and individual patient preferences should be considered when formulating a management plan for patients with IBS-D.
Keywords: alosetron; diarrhea; efficacy; eluxadoline; irritable bowel syndrome; rifaximin; safety; treatment.
© The Author(s), 2019.
Conflict of interest statement
Conflict of interest statement: DJC reports having nothing to disclose. BEL reports serving as an advisory board member for Ironwood Pharmaceuticals, Inc., Salix Pharmaceuticals, and Forest Laboratories, a subsidiary of Allergan plc.
Figures
References
-
- Lacy BE, Mearin F, Chang L, et al. Bowel disorders. Gastroenterology 2016; 150: 1393–1407. - PubMed
-
- Ringel Y, Williams RE, Kalilani L, et al. Prevalence, characteristics, and impact of bloating symptoms in patients with irritable bowel syndrome. Clin Gastroenterol Hepatol 2009; 7: 68–72. - PubMed
-
- Ballou S, Alhassan E, Hon E, et al. Sleep disturbances are commonly reported among patients presenting to a gastroenterology clinic. Dig Dis Sci 2018; 63: 2983–2991. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
