

Interrater Reliability of Experts in Identifying Interictal Epileptiform Discharges in Electroencephalograms
- PMID: 31633742
- PMCID: PMC6806666
- DOI: 10.1001/jamaneurol.2019.3531
Interrater Reliability of Experts in Identifying Interictal Epileptiform Discharges in Electroencephalograms
Erratum in
-
Incomplete Author Name and Credentials in Byline.JAMA Neurol. 2020 Jan 1;77(1):135. doi: 10.1001/jamaneurol.2019.4541. JAMA Neurol. 2020. PMID: 31930366 Free PMC article. No abstract available.
Abstract
Importance: The validity of using electroencephalograms (EEGs) to diagnose epilepsy requires reliable detection of interictal epileptiform discharges (IEDs). Prior interrater reliability (IRR) studies are limited by small samples and selection bias.
Objective: To assess the reliability of experts in detecting IEDs in routine EEGs.
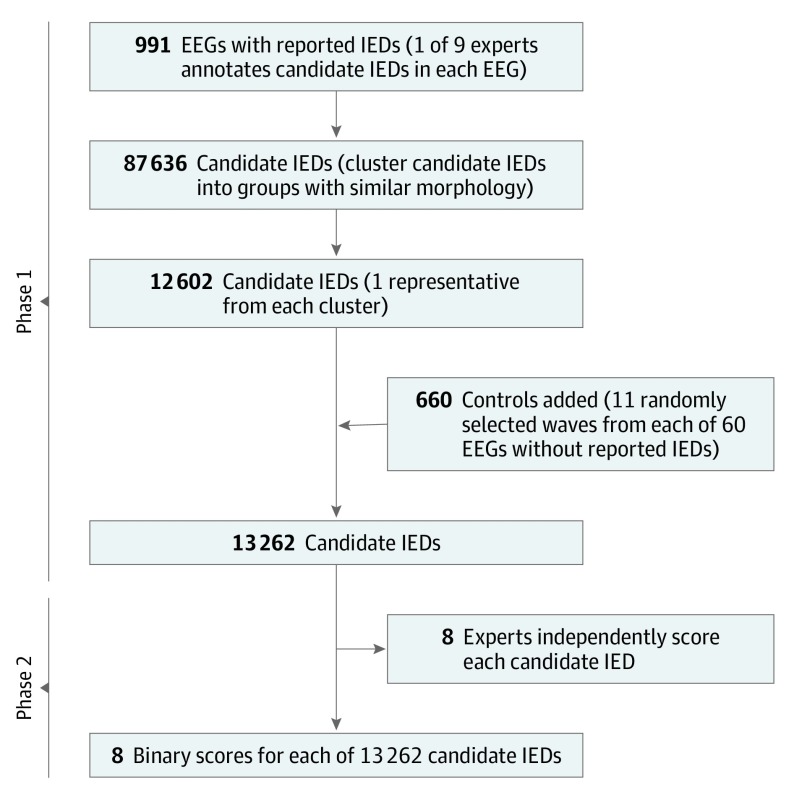
Design, setting, and participants: This prospective analysis conducted in 2 phases included as participants physicians with at least 1 year of subspecialty training in clinical neurophysiology. In phase 1, 9 experts independently identified candidate IEDs in 991 EEGs (1 expert per EEG) reported in the medical record to contain at least 1 IED, yielding 87 636 candidate IEDs. In phase 2, the candidate IEDs were clustered into groups with distinct morphological features, yielding 12 602 clusters, and a representative candidate IED was selected from each cluster. We added 660 waveforms (11 random samples each from 60 randomly selected EEGs reported as being free of IEDs) as negative controls. Eight experts independently scored all 13 262 candidates as IEDs or non-IEDs. The 1051 EEGs in the study were recorded at the Massachusetts General Hospital between 2012 and 2016.
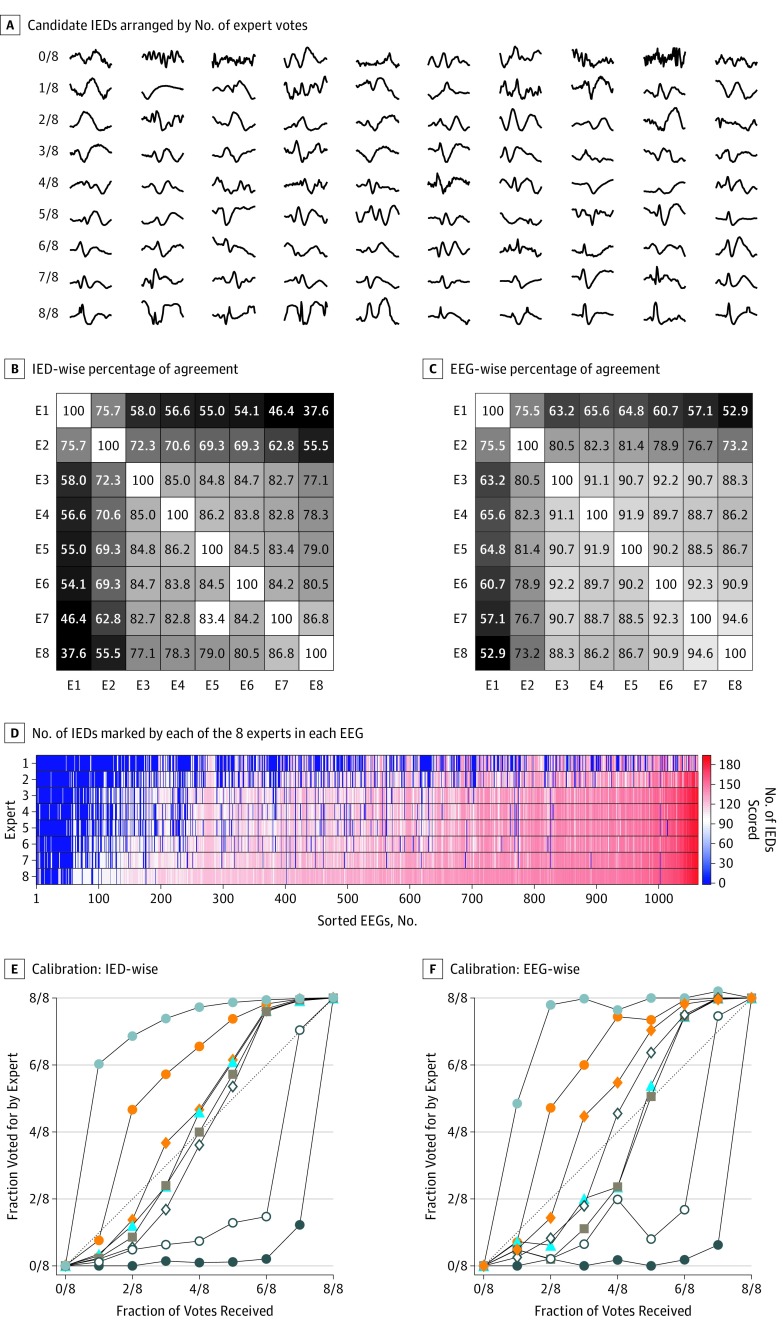
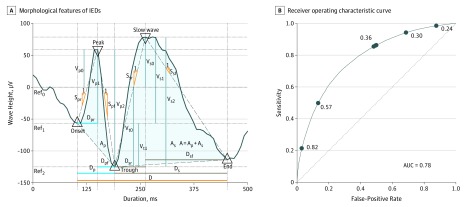
Main outcomes and measures: Primary outcome measures were percentage of agreement (PA) and beyond-chance agreement (Gwet κ) for individual IEDs (IED-wise IRR) and for whether an EEG contained any IEDs (EEG-wise IRR). Secondary outcomes were the correlations between numbers of IEDs marked by experts across cases, calibration of expert scoring to group consensus, and receiver operating characteristic analysis of how well multivariate logistic regression models may account for differences in the IED scoring behavior between experts.
Results: Among the 1051 EEGs assessed in the study, 540 (51.4%) were those of females and 511 (48.6%) were those of males. In phase 1, 9 experts each marked potential IEDs in a median of 65 (interquartile range [IQR], 28-332) EEGs. The total number of IED candidates marked was 87 636. Expert IRR for the 13 262 individually annotated IED candidates was fair, with the mean PA being 72.4% (95% CI, 67.0%-77.8%) and mean κ being 48.7% (95% CI, 37.3%-60.1%). The EEG-wise IRR was substantial, with the mean PA being 80.9% (95% CI, 76.2%-85.7%) and mean κ being 69.4% (95% CI, 60.3%-78.5%). A statistical model based on waveform morphological features, when provided with individualized thresholds, explained the median binary scores of all experts with a high degree of accuracy of 80% (range, 73%-88%).
Conclusions and relevance: This study's findings suggest that experts can identify whether EEGs contain IEDs with substantial reliability. Lower reliability regarding individual IEDs may be largely explained by various experts applying different thresholds to a common underlying statistical model.
Conflict of interest statement
Figures
Comment in
-
Most Experts Agree … But What About Other EEG Readers?Epilepsy Curr. 2020 Feb 17;20(2):78-79. doi: 10.1177/1535759720901511. eCollection 2020 Mar-Apr. Epilepsy Curr. 2020. PMID: 32313500 Free PMC article. No abstract available.
