

Metoprolol for the Prevention of Acute Exacerbations of COPD
- PMID: 31633896
- PMCID: PMC7416529
- DOI: 10.1056/NEJMoa1908142
Metoprolol for the Prevention of Acute Exacerbations of COPD
Abstract
Background: Observational studies suggest that beta-blockers may reduce the risk of exacerbations and death in patients with moderate or severe chronic obstructive pulmonary disease (COPD), but these findings have not been confirmed in randomized trials.
Methods: In this prospective, randomized trial, we assigned patients between the ages of 40 and 85 years who had COPD to receive either a beta-blocker (extended-release metoprolol) or placebo. All the patients had a clinical history of COPD, along with moderate airflow limitation and an increased risk of exacerbations, as evidenced by a history of exacerbations during the previous year or the prescribed use of supplemental oxygen. We excluded patients who were already taking a beta-blocker or who had an established indication for the use of such drugs. The primary end point was the time until the first exacerbation of COPD during the treatment period, which ranged from 336 to 350 days, depending on the adjusted dose of metoprolol.
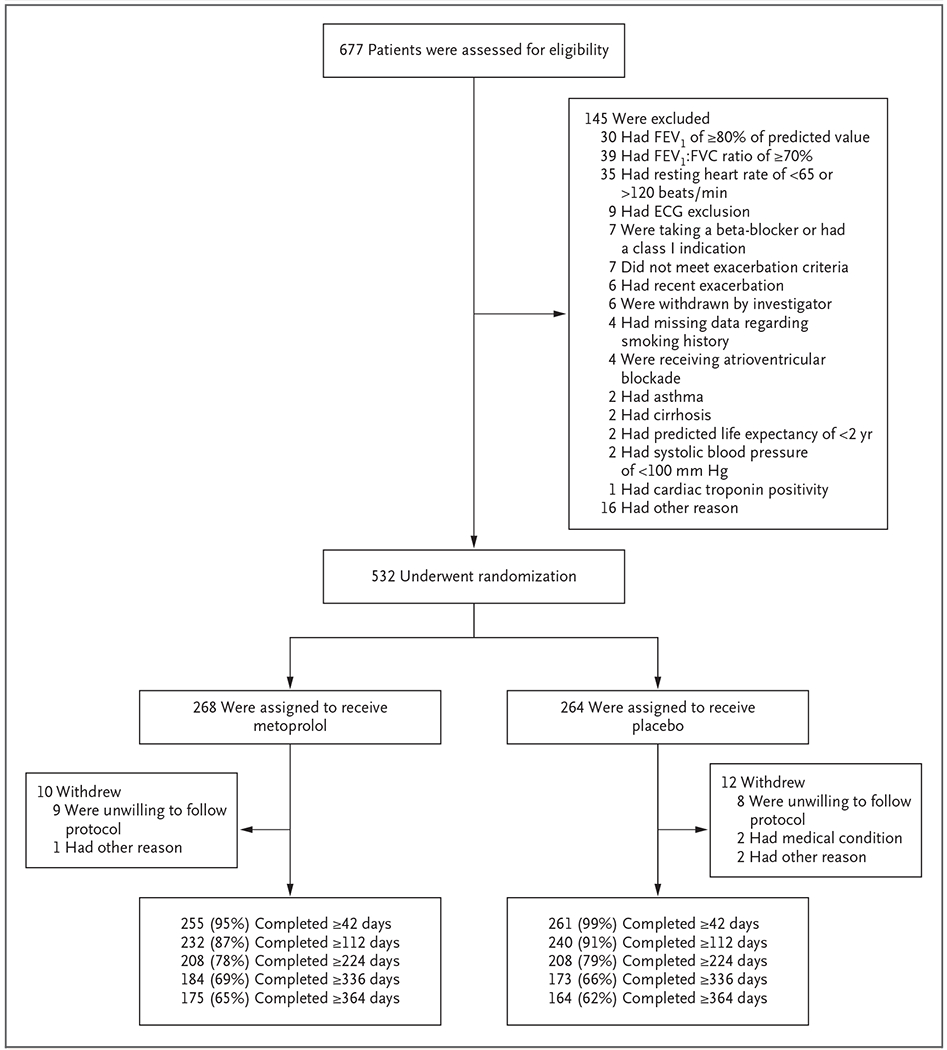
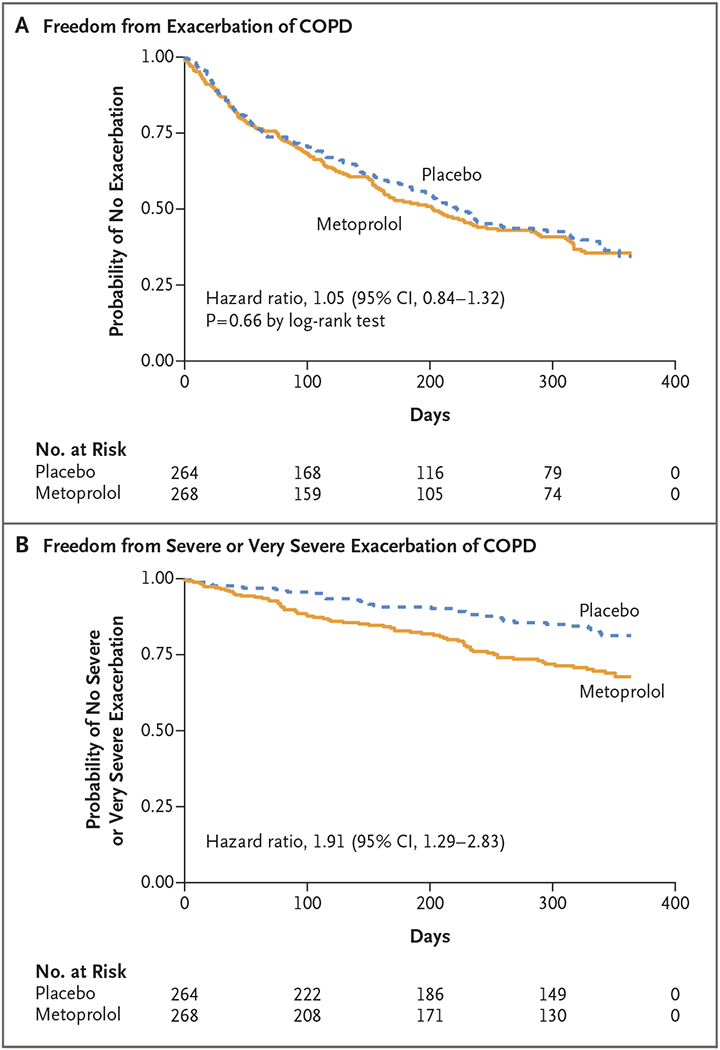
Results: A total of 532 patients underwent randomization. The mean (±SD) age of the patients was 65.0±7.8 years; the mean forced expiratory volume in 1 second (FEV1) was 41.1±16.3% of the predicted value. The trial was stopped early because of futility with respect to the primary end point and safety concerns. There was no significant between-group difference in the median time until the first exacerbation, which was 202 days in the metoprolol group and 222 days in the placebo group (hazard ratio for metoprolol vs. placebo, 1.05; 95% confidence interval [CI], 0.84 to 1.32; P = 0.66). Metoprolol was associated with a higher risk of exacerbation leading to hospitalization (hazard ratio, 1.91; 95% CI, 1.29 to 2.83). The frequency of side effects that were possibly related to metoprolol was similar in the two groups, as was the overall rate of nonrespiratory serious adverse events. During the treatment period, there were 11 deaths in the metoprolol group and 5 in the placebo group.
Conclusions: Among patients with moderate or severe COPD who did not have an established indication for beta-blocker use, the time until the first COPD exacerbation was similar in the metoprolol group and the placebo group. Hospitalization for exacerbation was more common among the patients treated with metoprolol. (Funded by the Department of Defense; BLOCK COPD ClinicalTrials.gov number, NCT02587351.).
Copyright © 2019 Massachusetts Medical Society.
Figures
Comment in
-
Beta-Blockers in COPD - A Controversy Resolved?N Engl J Med. 2019 Dec 12;381(24):2367-2368. doi: 10.1056/NEJMe1912664. Epub 2019 Oct 20. N Engl J Med. 2019. PMID: 31633892 No abstract available.
-
Metoprolol for the Prevention of Exacerbations of COPD.N Engl J Med. 2020 Apr 2;382(14):1374. doi: 10.1056/NEJMc2000638. N Engl J Med. 2020. PMID: 32242367 No abstract available.
-
Metoprolol for the Prevention of Exacerbations of COPD.N Engl J Med. 2020 Apr 2;382(14):1374-1375. doi: 10.1056/NEJMc2000638. N Engl J Med. 2020. PMID: 32242368 No abstract available.
-
Metoprolol for the Prevention of Exacerbations of COPD.N Engl J Med. 2020 Apr 2;382(14):1375. doi: 10.1056/NEJMc2000638. N Engl J Med. 2020. PMID: 32242369 No abstract available.
References
-
- Vogelmeier CF, Criner GJ, Martinez FJ, et al. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Lung Disease 2017 Report: GOLD executive summary. Am J Respir Crit Care Med 2017;195:557–82. - PubMed
-
- Bhatt SP, Dransfield MT. Chronic obstructive pulmonary disease and cardiovascular disease. Transl Res 2013;162:237–51. - PubMed
-
- Chen W, Thomas J, Sadatsafavi M, FitzGerald JM. Risk of cardiovascular comorbidity in patients with chronic obstructive pulmonary disease: a systematic review and meta-analysis. Lancet Respir Med 2015;3:631–9. - PubMed