

Incidence and Outcomes of Acute Laryngeal Injury After Prolonged Mechanical Ventilation
- PMID: 31634236
- PMCID: PMC7880159
- DOI: 10.1097/CCM.0000000000004015
Incidence and Outcomes of Acute Laryngeal Injury After Prolonged Mechanical Ventilation
Abstract
Objectives: Upper airway injury is a recognized complication of prolonged endotracheal intubation, yet little attention has been paid to the consequences of laryngeal injury and functional impact. The purpose of our study was to prospectively define the incidence of acute laryngeal injury and investigate the impact of injury on breathing and voice outcomes.
Design: Prospective cohort study.
Setting: Tertiary referral critical care center.
Patients: Consecutive adult patients intubated greater than 12 hours in the medical ICU from August 2017 to May 2018 who underwent laryngoscopy within 36 hours of extubation.
Interventions: Laryngoscopy following endotracheal intubation.
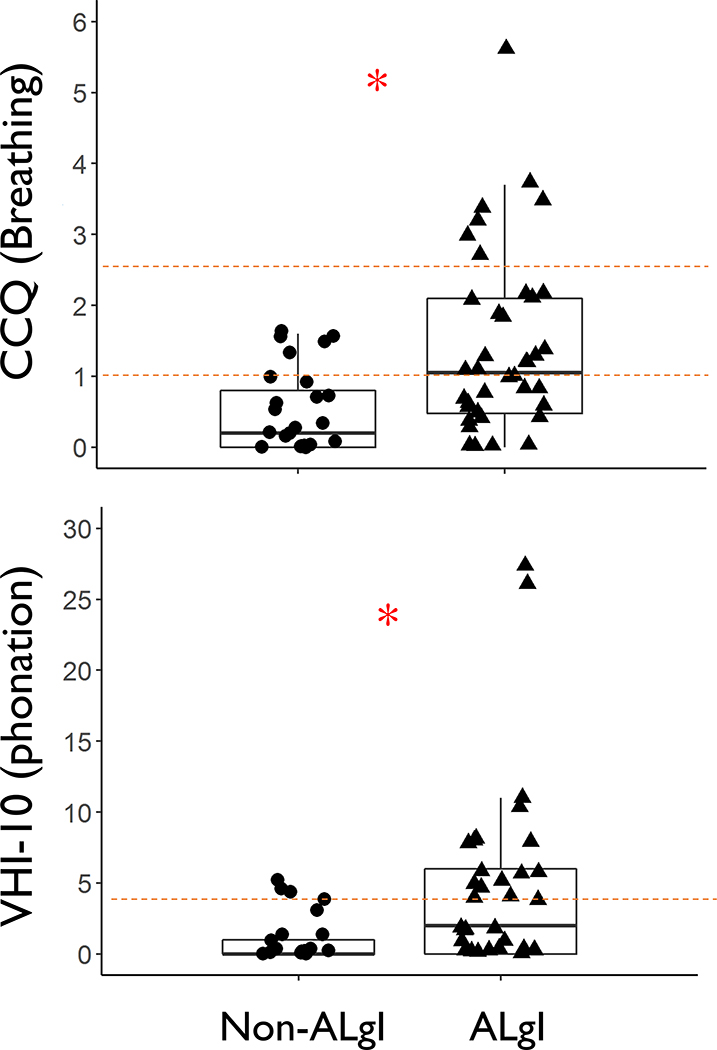
Measurements and main results: One hundred consecutive patients (62% male; median age, 58.5 yr) underwent endoscopic examination after extubation. Acute laryngeal injury (i.e., mucosal ulceration or granulation tissue in the larynx) was present in 57 patients (57%). Patients with laryngeal injury had significantly worse patient-reported breathing (Clinical Chronic Obstructive Pulmonary Disease Questionnaire: median, 1.05; interquartile range, 0.48-2.10) and vocal symptoms (Voice Handicap Index-10: median, 2; interquartile range, 0-6) compared with patients without injury (Clinical Chronic Obstructive Pulmonary Disease Questionnaire: median, 0.20; interquartile range, 0-0.80; p < 0.001; and Voice Handicap Index-10: median, 0; interquartile range, 0-1; p = 0.005). Multivariable logistic regression independently associated diabetes, body habitus, and endotracheal tube size greater than 7.0 with the development of laryngeal injury.
Conclusions: Acute laryngeal injury occurs in more than half of patients who receive mechanical ventilation and is associated with significantly worse breathing and voicing 10 weeks after extubation. An endotracheal tube greater than size 7.0, diabetes, and larger body habitus may predispose to injury. Our results suggest that acute laryngeal injury impacts functional recovery from critical illness.
Trial registration: ClinicalTrials.gov NCT03250975.
Figures


Comment in
-
Acute Laryngeal Injury Following Mechanical Ventilation: Revisiting the Known Unknowns.Crit Care Med. 2019 Dec;47(12):1802-1804. doi: 10.1097/CCM.0000000000004049. Crit Care Med. 2019. PMID: 31738247 No abstract available.
-
Preventing Lungs and Larynx Injury by Low Tidal Volume and Small Size Endotracheal Tube: Are We Really Hurting a Lot?Crit Care Med. 2020 Apr;48(4):e338. doi: 10.1097/CCM.0000000000004216. Crit Care Med. 2020. PMID: 32205632 No abstract available.
-
The authors reply.Crit Care Med. 2020 Apr;48(4):e338-e339. doi: 10.1097/CCM.0000000000004253. Crit Care Med. 2020. PMID: 32205633 No abstract available.
-
Understanding Variable Prevalences of Acute Laryngeal Injury Post-Extubation.Crit Care Med. 2020 May;48(5):e430-e431. doi: 10.1097/CCM.0000000000004245. Crit Care Med. 2020. PMID: 32301782 No abstract available.
-
The authors reply.Crit Care Med. 2020 May;48(5):e431. doi: 10.1097/CCM.0000000000004301. Crit Care Med. 2020. PMID: 32301783 No abstract available.
References
-
- Angus DC, Shorr AF, White A, et al.: Critical care delivery in the United States: distribution of services and compliance with Leapfrog recommendations. Crit Care Med 2006;34(4):1016–1024. - PubMed
-
- Angus DC, Linde-Zwirble WT, Lidicker J, et al.: Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care. Crit Care Med 2001;29(7):1303–1310. - PubMed
-
- Ashiku SK, Kuzucu A, Grillo HC, et al.: Idiopathic laryngotracheal stenosis: effective definitive treatment with laryngotracheal resection. J Thorac Cardiovasc Surg 2004;127(1):99–107. - PubMed
-
- Needham DM, Davidson J, Cohen H, et al.: Improving long-term outcomes after discharge from intensive care unit: report from a stakeholders’ conference. Crit Care Med 2012;40(2):502–509. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
