

Morbidity and Mortality After Surgery for Nonmalignant Colorectal Polyps: A 10-Year Nationwide Analysis
- PMID: 31634261
- PMCID: PMC6830963
- DOI: 10.14309/ajg.0000000000000407
Morbidity and Mortality After Surgery for Nonmalignant Colorectal Polyps: A 10-Year Nationwide Analysis
Abstract
Objectives: Rates of surgery for nonmalignant colorectal polyps are increasing in the United States despite evidence that most polyps can be managed endoscopically. We aimed to determine nationally representative estimates and to identify predictors of in-hospital mortality and morbidity after surgery for nonmalignant colorectal polyps.
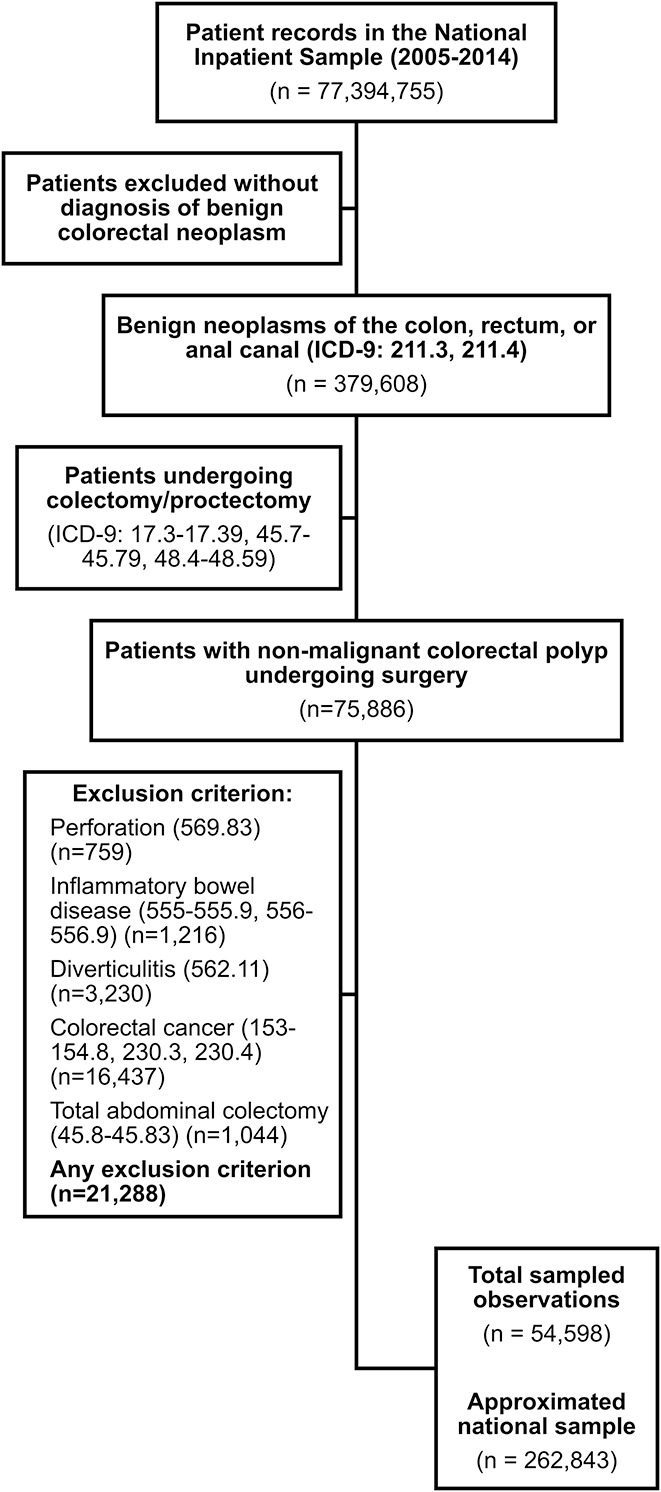
Methods: Data were analyzed from the National Inpatient Sample for 2005-2014. All discharges for adult patients undergoing surgery for nonmalignant colorectal polyps were identified. Rates of in-hospital mortality and postoperative wound, infectious, urinary, pulmonary, gastrointestinal, or cardiovascular adverse events were calculated. Multivariable logistic regression using survey-weighted data was used to evaluate covariables associated with postoperative mortality and morbidity.
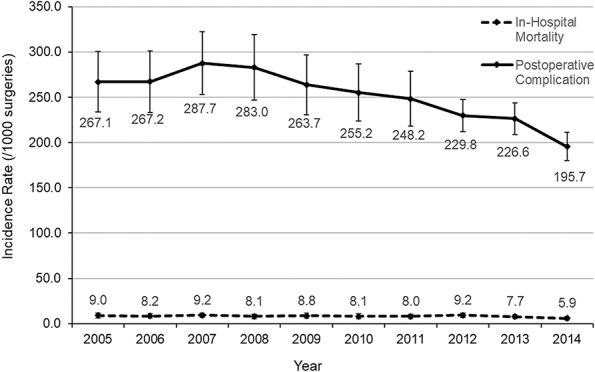
Results: An estimated 262,843 surgeries for nonmalignant colorectal polyps were analyzed. In-hospital mortality was 0.8% [95% confidence interval: 0.7%-0.9%] and morbidity was 25.3% [95% confidence interval: 24.2%-26.4%]. Postoperative mortality was associated with open surgical technique (vs laparoscopic), older age, black race (vs non-Hispanic white), Medicaid use, and burden of comorbidities. Female sex and private insurance were associated with lower risk. Patients developing a postoperative adverse event had a 106% increase in mean hospital length of stay (10.3 vs 5.0 days; P < 0.0001) and 91% increase in mean hospitalization cost ($77,015.24 vs $40,258.30; P < 0.0001).
Discussion: Surgery for nonmalignant colorectal polyps is associated with almost 1% mortality and common morbidity. These findings should inform risk vs benefit discussions for clinicians and patients, and although confounding by patient selection cannot be excluded, the risks associated with surgery support consideration of endoscopic resection as a potentially less invasive therapeutic option.
Figures
References
-
- Heitman SJ, Tate DJ, Bourke MJ. Optimizing resection of large colorectal polyps. Curr Treat Options Gastroenterol 2017;15:213–29. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
