

Presurgical evaluation of basal cell carcinoma using combined reflectance confocal microscopy-optical coherence tomography: A prospective study
- PMID: 31634517
- PMCID: PMC7513586
- DOI: 10.1016/j.jaad.2019.10.028
Presurgical evaluation of basal cell carcinoma using combined reflectance confocal microscopy-optical coherence tomography: A prospective study
Abstract
Background: Initial biopsy of basal cell carcinoma (BCC) may fail to show aggressive histologic subtypes. Additionality, the clinical evaluation of BCC before surgery can miss subclinical extension. Reflectance confocal microscopy (RCM) and optical coherence tomography (OCT) are emerging tools that can help in the presurgical evaluation of BCCs.
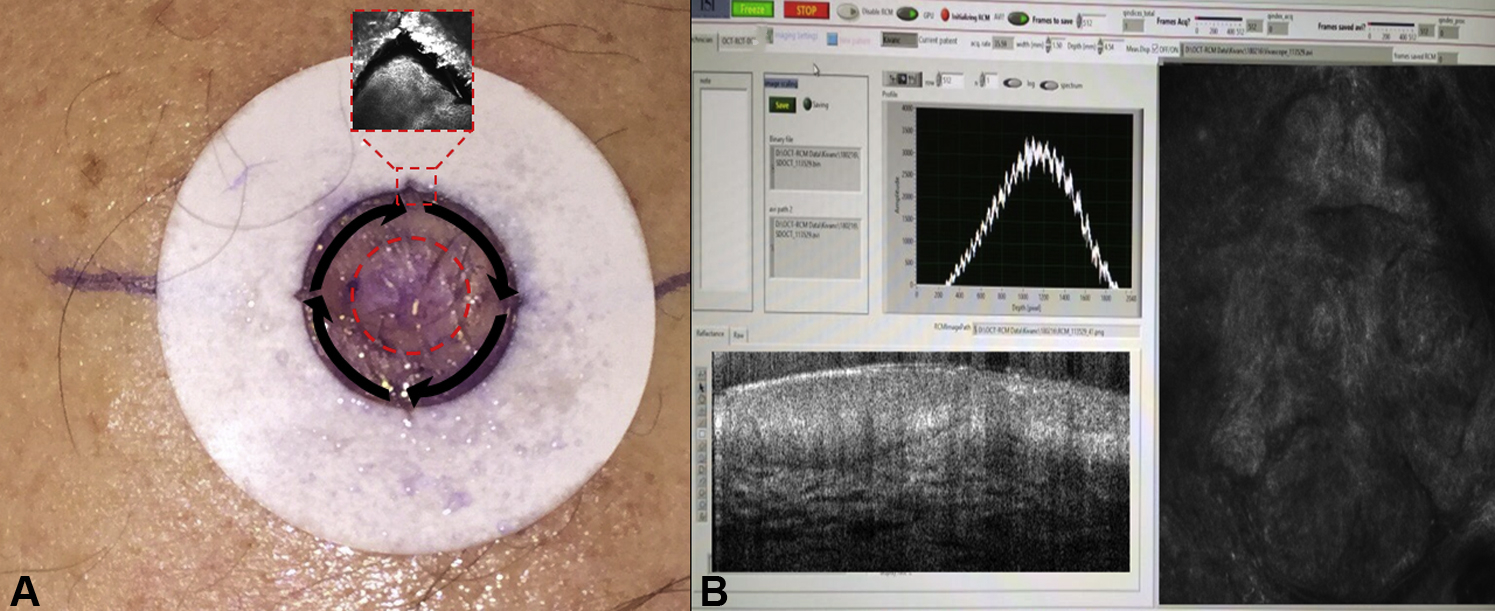
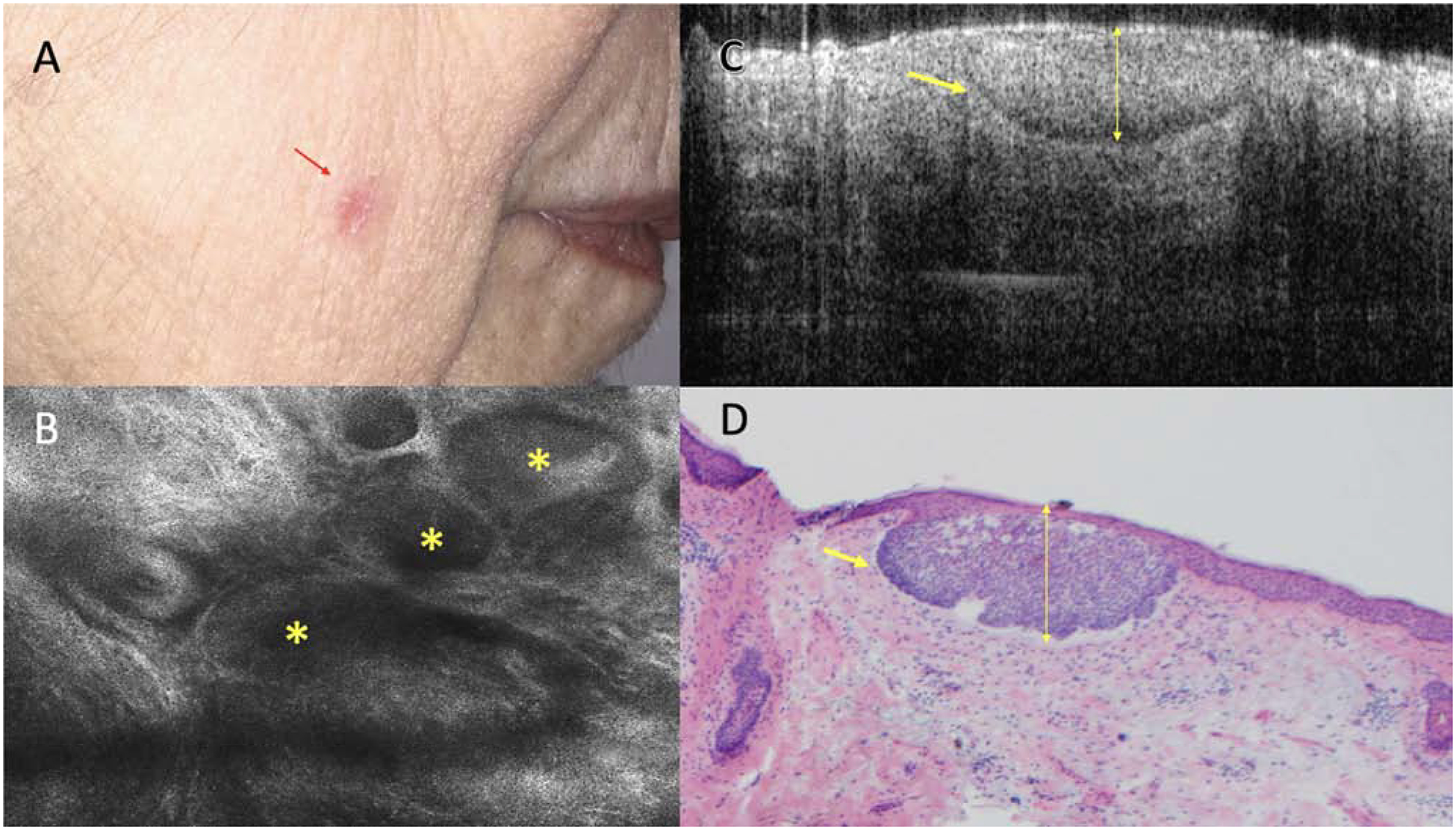
Objective: To assess the feasibility of a combined RCM-OCT imaging modality for presurgical evaluation of biopsy-proven BCCs for residual tumor, margin status, and depth.
Methods: Thirty-eight BCCs in 35 patients referred to a tertiary cancer center for Mohs micrographic surgery (MMS) were imaged with combined RCM-OCT. Images were correlated to MMS frozen sections.
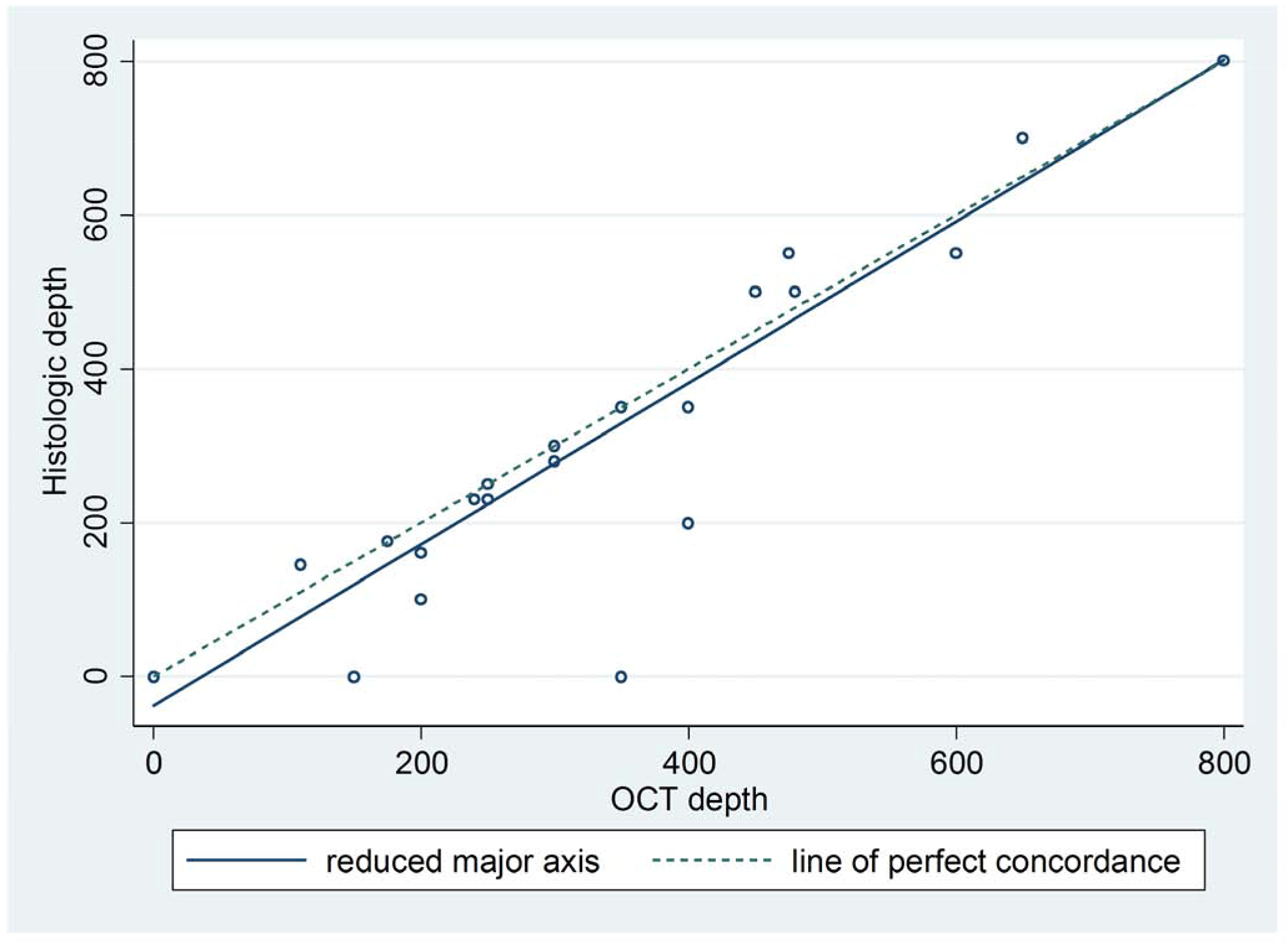
Results: Thirty-eight BCCs were analyzed. The mean age of patients was 67.34 years (range, 36-84 years), and 20 patients were female (57.14%). Twenty four BCCs were located on the head (63.16%) , and the mean size was 8.58 mm (range, 3-30 mm). RCM-OCT showed an overall agreement of 91.1% with MMS frozen sections. A sensitivity of 82.6% (95% confidence interval [CI], 69%-92%), specificity of 93.8% (95% CI, 88%-97%), and receiver operating characteristic curve of 0.88 (95% CI, 0.82-0.94) was found. OCT depth was highly correlated with MMS depth (r2 = 0.9).
Limitations: Small sample size and difficulty evaluating certain challenging anatomic sites.
Conclusions: Combined RCM-OCT may emerge as a useful tool for presurgical evaluation of BCCs.
Keywords: Mohs; basal cell carcinoma; biopsy; margins; optical coherence tomography; reflectance confocal microscopy; residual; surgery.
Copyright © 2019 American Academy of Dermatology, Inc. Published by Elsevier Inc. All rights reserved.
Figures

Similar articles
-
Management of complex head-and-neck basal cell carcinomas using a combined reflectance confocal microscopy/optical coherence tomography: a descriptive study.Arch Dermatol Res. 2021 Apr;313(3):193-200. doi: 10.1007/s00403-020-02037-6. Epub 2020 Feb 4. Arch Dermatol Res. 2021. PMID: 32020324 Free PMC article.
-
Evaluation of a Combined Reflectance Confocal Microscopy-Optical Coherence Tomography Device for Detection and Depth Assessment of Basal Cell Carcinoma.JAMA Dermatol. 2018 Oct 1;154(10):1175-1183. doi: 10.1001/jamadermatol.2018.2446. JAMA Dermatol. 2018. PMID: 30140851 Free PMC article.
-
Reflectance confocal microscopy confirms residual basal cell carcinoma on clinically negative biopsy sites before Mohs micrographic surgery: A prospective study.J Am Acad Dermatol. 2019 Aug;81(2):417-426. doi: 10.1016/j.jaad.2019.02.049. Epub 2019 Jun 19. J Am Acad Dermatol. 2019. PMID: 31227277 Free PMC article.
-
Novel imaging techniques for tumor margin detection in basal cell carcinoma: a systematic scoping review of FDA and EMA-approved imaging modalities.Int J Dermatol. 2025 Feb;64(2):287-301. doi: 10.1111/ijd.17496. Epub 2024 Oct 2. Int J Dermatol. 2025. PMID: 39358676 Free PMC article.
-
Mohs micrographic surgery challenges and new technologies to optimize care of cutaneous malignancies of the ear.Arch Dermatol Res. 2024 Jun 1;316(6):320. doi: 10.1007/s00403-024-03127-5. Arch Dermatol Res. 2024. PMID: 38822894 Review.
Cited by
-
Management of periocular keratinocyte carcinomas with Mohs micrographic surgery and predictors of complex reconstruction: a retrospective study.An Bras Dermatol. 2024 Mar-Apr;99(2):202-209. doi: 10.1016/j.abd.2023.05.004. Epub 2023 Nov 20. An Bras Dermatol. 2024. PMID: 37989688 Free PMC article.
-
Combining Reflectance Confocal Microscopy, Optical Coherence Tomography and Ex-Vivo Fluorescence Confocal Microscopy for Margin Assessment in Basal Cell Carcinoma Excision.Dermatol Pract Concept. 2024 Apr 1;14(2):e2024090. doi: 10.5826/dpc.1402a90. Dermatol Pract Concept. 2024. PMID: 38810079 Free PMC article.
-
Cancer: a mirrored room between tumor bulk and tumor microenvironment.J Exp Clin Cancer Res. 2021 Jun 28;40(1):217. doi: 10.1186/s13046-021-02022-5. J Exp Clin Cancer Res. 2021. PMID: 34183054 Free PMC article. Review.
-
Angulated small nests and cords: Key diagnostic histopathologic features of infiltrative basal cell carcinoma can be identified using integrated reflectance confocal microscopy-optical coherence tomography.J Cutan Pathol. 2021 Jan;48(1):53-65. doi: 10.1111/cup.13871. Epub 2020 Oct 12. J Cutan Pathol. 2021. PMID: 32989842 Free PMC article.
-
Confocal Microscopy for Diagnosis and Management of Cutaneous Malignancies: Clinical Impacts and Innovation.Diagnostics (Basel). 2023 Feb 23;13(5):854. doi: 10.3390/diagnostics13050854. Diagnostics (Basel). 2023. PMID: 36899999 Free PMC article. Review.
References
-
- Lomas A, Leonardi-Bee J, Bath-Hextall F. A systematic review of worldwide incidence of nonmelanoma skin cancer. Br J Dermatol 2012;166:1069–80. - PubMed
-
- Rogers HW, Weinstock MA, Feldman SR, Coldiron BM. Incidence Estimate of Nonmelanoma Skin Cancer (Keratinocyte Carcinomas) in the U.S. Population, 2012. JAMA Dermatol 2015;151:1081–6. - PubMed
-
- Drucker AM, Adam GP, Rofeberg V, Gazula A, Smith B, Moustafa F et al. Treatments of Primary Basal Cell Carcinoma of the Skin: A Systematic Review and Network Meta-analysis. Ann Intern Med 2018;169:456–66. - PubMed
-
- National Comprehensive Cancer Network. Melanoma (Version 2.2018).
-
- Sasor SE, Nosrati NN, Katona T, Wooden WA, Cohen A, Munshi IA et al. Predicting the Presence of Nonmelanoma Skin Cancers After Biopsy: A Method to Reduce Unnecessary Surgical Procedures. JAMA Surg 2016;151:289–90. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
