

Modular design of a tissue engineered pulsatile conduit using human induced pluripotent stem cell-derived cardiomyocytes
- PMID: 31634626
- PMCID: PMC7227659
- DOI: 10.1016/j.actbio.2019.10.019
Modular design of a tissue engineered pulsatile conduit using human induced pluripotent stem cell-derived cardiomyocytes
Abstract
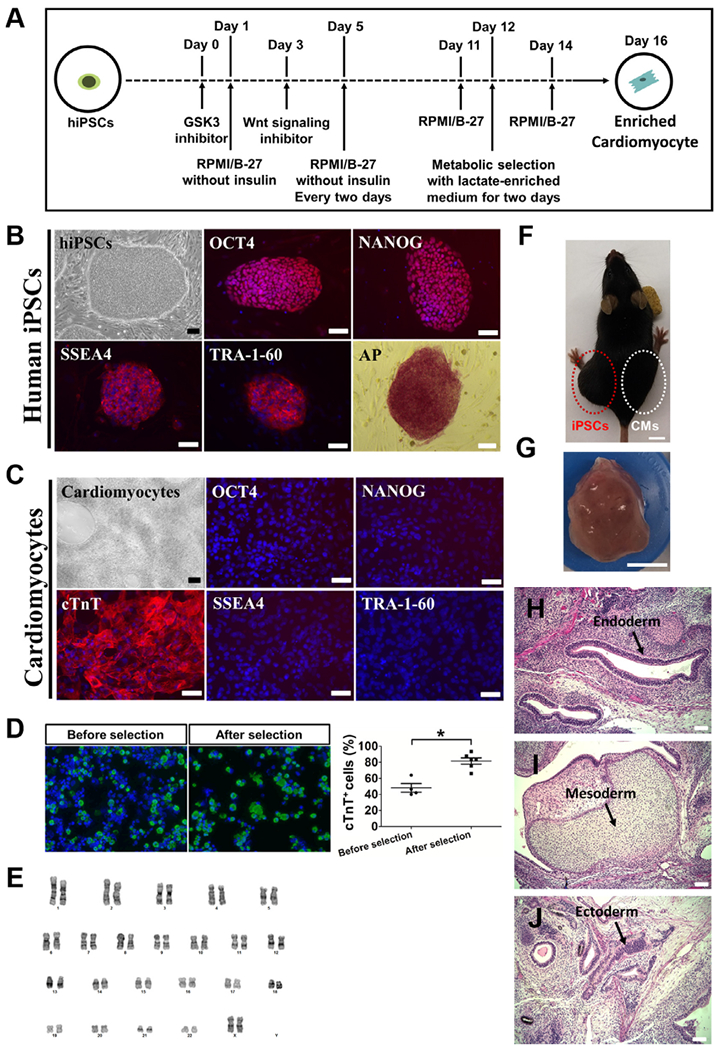
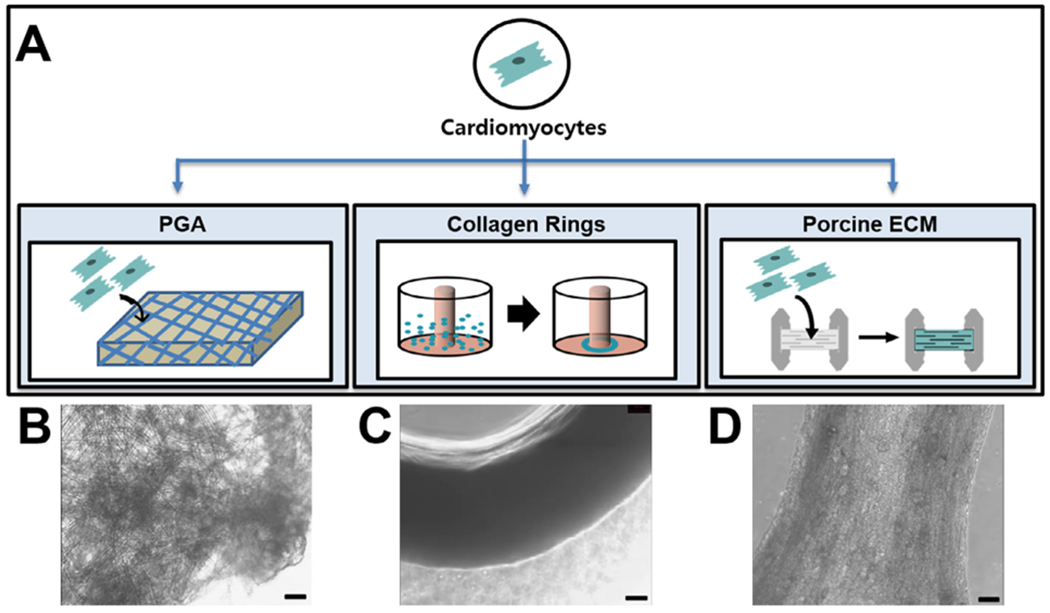
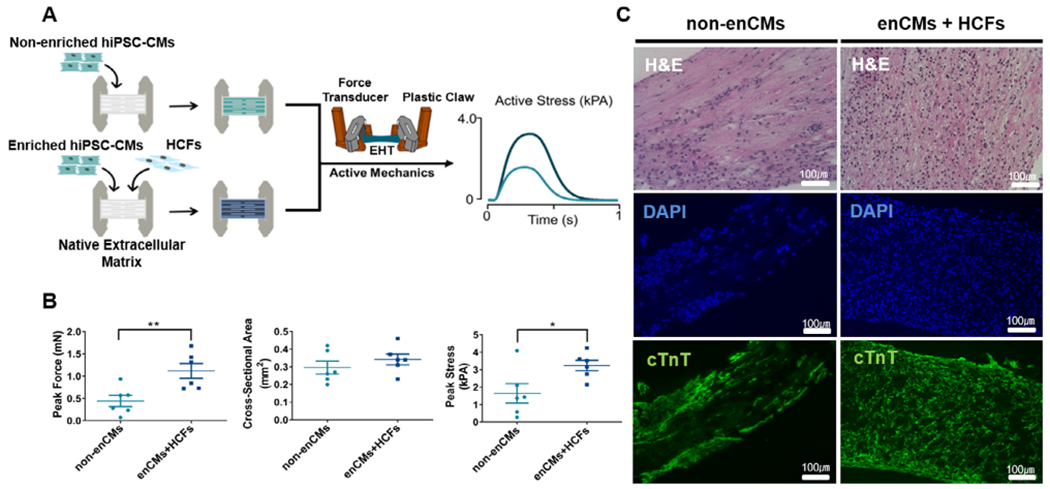
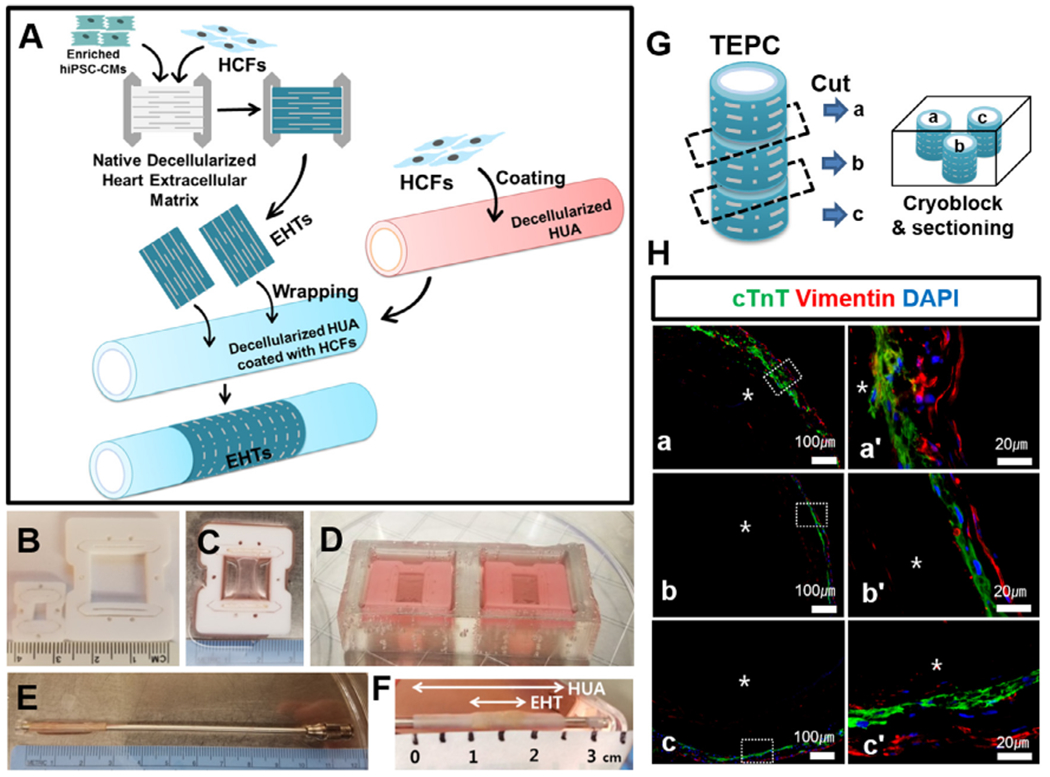
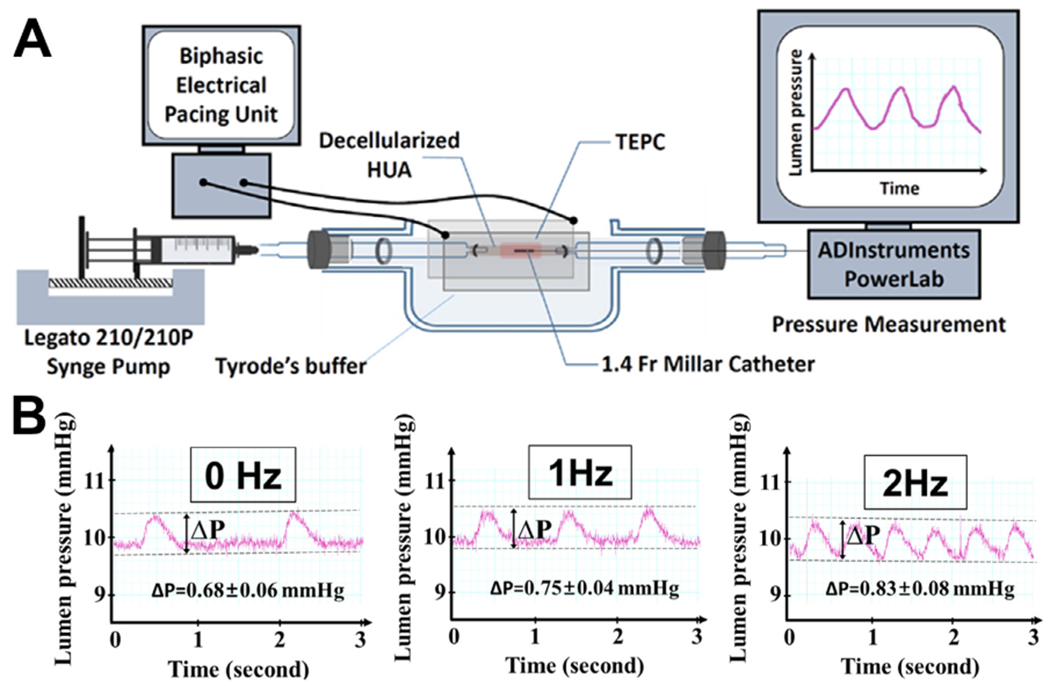
Single ventricle heart defects (SVDs) are congenital disorders that result in a variety of complications, including increased ventricular mechanical strain and mixing of oxygenated and deoxygenated blood, leading to heart failure without surgical intervention. Corrective surgery for SVDs are traditionally handled by the Fontan procedure, requiring a vascular conduit for completion. Although effective, current conduits are limited by their inability to aid in pumping blood into the pulmonary circulation. In this report, we propose an innovative and versatile design strategy for a tissue engineered pulsatile conduit (TEPC) to aid circulation through the pulmonary system by producing contractile force. Several design strategies were tested for production of a functional TEPC. Ultimately, we found that porcine extracellular matrix (ECM)-based engineered heart tissue (EHT) composed of human induced pluripotent stem cell-derived cardiomyocytes (hiPSC-CMs) and primary cardiac fibroblasts (HCF) wrapped around decellularized human umbilical artery (HUA) made an efficacious basal TEPC. Importantly, the TEPCs showed effective electrical and mechanical function. Initial pressure readings from our TEPC in vitro (0.68 mmHg) displayed efficient electrical conductivity enabling them to follow electrical pacing up to a 2 Hz frequency. This work represents a proof of principle study for our current TEPC design strategy. Refinement and optimization of this promising TEPC design will lay the groundwork for testing the construct's therapeutic potential in the future. Together this work represents a progressive step toward developing an improved treatment for SVD patients. STATEMENT OF SIGNIFICANCE: Single Ventricle Cardiac defects (SVD) are a form of congenital disorder with a morbid prognosis without surgical intervention. These patients are treated through the Fontan procedure which requires vascular conduits to complete. Fontan conduits have been traditionally made from stable or biodegradable materials with no pumping activity. Here, we propose a tissue engineered pulsatile conduit (TEPC) for use in Fontan circulation to alleviate excess strain in SVD patients. In contrast to previous strategies for making a pulsatile Fontan conduit, we employ a modular design strategy that allows for the optimization of each component individually to make a standalone tissue. This work sets the foundation for an in vitro, trainable human induced pluripotent stem cell based TEPC.
Keywords: Engineered heart tissue; Fontan Conduit; Human induced pluripotent stem cells; TEPC; Tissue engineering.
Copyright © 2019. Published by Elsevier Ltd.
Conflict of interest statement
Declaration of Competing Interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
Similar articles
-
Advanced tissue-engineered pulsatile conduit using human induced pluripotent stem cell-derived cardiomyocytes.Acta Biomater. 2025 Jun 27:S1742-7061(25)00475-1. doi: 10.1016/j.actbio.2025.06.055. Online ahead of print. Acta Biomater. 2025. PMID: 40582540
-
Engineered heart tissue models from hiPSC-derived cardiomyocytes and cardiac ECM for disease modeling and drug testing applications.Acta Biomater. 2019 Jul 1;92:145-159. doi: 10.1016/j.actbio.2019.05.016. Epub 2019 May 7. Acta Biomater. 2019. PMID: 31075518
-
Enhanced elastin synthesis and maturation in human vascular smooth muscle tissue derived from induced-pluripotent stem cells.Acta Biomater. 2017 Apr 1;52:49-59. doi: 10.1016/j.actbio.2017.01.083. Epub 2017 Feb 3. Acta Biomater. 2017. PMID: 28163239
-
Modeling Cardiovascular Diseases with hiPSC-Derived Cardiomyocytes in 2D and 3D Cultures.Int J Mol Sci. 2020 May 11;21(9):3404. doi: 10.3390/ijms21093404. Int J Mol Sci. 2020. PMID: 32403456 Free PMC article. Review.
-
Induced pluripotent stem cells for cardiac repair.Cell Mol Life Sci. 2012 Oct;69(19):3285-99. doi: 10.1007/s00018-012-1078-2. Epub 2012 Jul 20. Cell Mol Life Sci. 2012. PMID: 22960788 Free PMC article. Review.
Cited by
-
Muscle LIM Protein Force-Sensing Mediates Sarcomeric Biomechanical Signaling in Human Familial Hypertrophic Cardiomyopathy.Circulation. 2022 Apr 19;145(16):1238-1253. doi: 10.1161/CIRCULATIONAHA.121.056265. Epub 2022 Apr 6. Circulation. 2022. PMID: 35384713 Free PMC article.
-
Efficient Differentiation of Human Induced Pluripotent Stem Cells into Endothelial Cells under Xenogeneic-free Conditions for Vascular Tissue Engineering.Acta Biomater. 2021 Jan 1;119:184-196. doi: 10.1016/j.actbio.2020.11.007. Epub 2020 Nov 6. Acta Biomater. 2021. PMID: 33166710 Free PMC article.
-
Beyond Family: Modeling Non-hereditary Heart Diseases With Human Pluripotent Stem Cell-Derived Cardiomyocytes.Front Physiol. 2020 Apr 22;11:384. doi: 10.3389/fphys.2020.00384. eCollection 2020. Front Physiol. 2020. PMID: 32390874 Free PMC article. Review.
-
FRESH 3D bioprinting a contractile heart tube using human stem cell-derived cardiomyocytes.Biofabrication. 2022 Mar 16;14(2):10.1088/1758-5090/ac58be. doi: 10.1088/1758-5090/ac58be. Biofabrication. 2022. PMID: 35213846 Free PMC article.
-
Fabrication of heart tubes from iPSC derived cardiomyocytes and human fibrinogen by rotating mold technology.Sci Rep. 2024 Jun 7;14(1):13174. doi: 10.1038/s41598-024-64022-7. Sci Rep. 2024. PMID: 38849457 Free PMC article.
References
-
- Leary PWO, Prevalence, clinical presentation and natural history of patients with single ventricle, 16 (2002) 31–38.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
