

Effect of Fibrinogen Concentrate vs Cryoprecipitate on Blood Component Transfusion After Cardiac Surgery: The FIBRES Randomized Clinical Trial
- PMID: 31634905
- PMCID: PMC6822637
- DOI: 10.1001/jama.2019.17312
Effect of Fibrinogen Concentrate vs Cryoprecipitate on Blood Component Transfusion After Cardiac Surgery: The FIBRES Randomized Clinical Trial
Abstract
Importance: Excessive bleeding is a common complication of cardiac surgery. An important cause of bleeding is acquired hypofibrinogenemia (fibrinogen level <1.5-2.0 g/L), for which guidelines recommend fibrinogen replacement with cryoprecipitate or fibrinogen concentrate. The 2 products have important differences, but comparative clinical data are lacking.
Objective: To determine if fibrinogen concentrate is noninferior to cryoprecipitate for treatment of bleeding related to hypofibrinogenemia after cardiac surgery.
Design, setting, and participants: Randomized clinical trial at 11 Canadian hospitals enrolling adult patients experiencing clinically significant bleeding and hypofibrinogenemia after cardiac surgery (from February 10, 2017, to November 1, 2018). Final 28-day follow-up visit was completed on November 28, 2018.
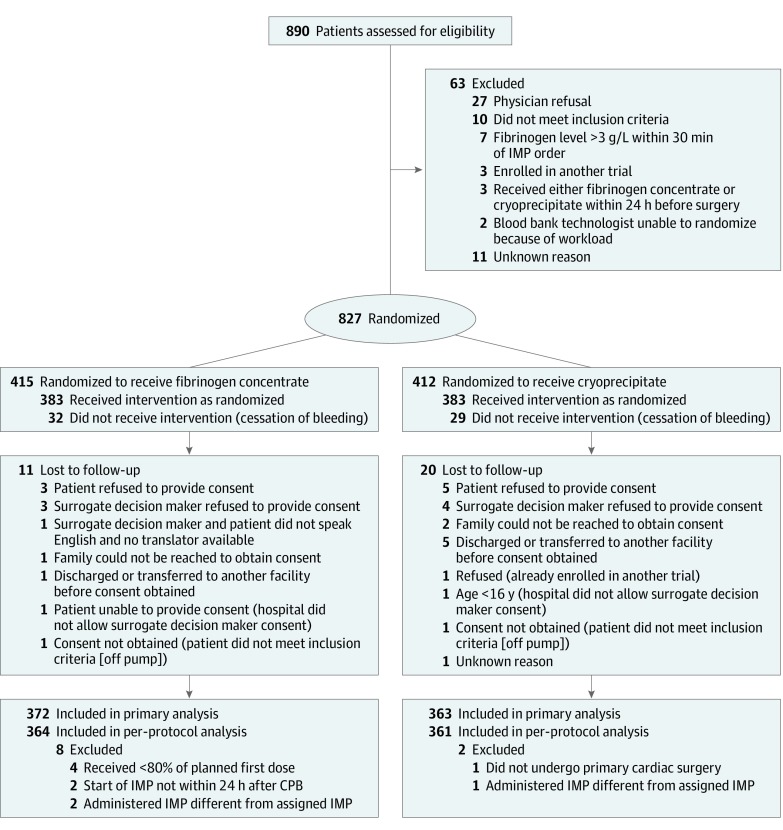
Interventions: Fibrinogen concentrate (4 g; n = 415) or cryoprecipitate (10 units; n = 412) for each ordered dose within 24 hours after cardiopulmonary bypass.
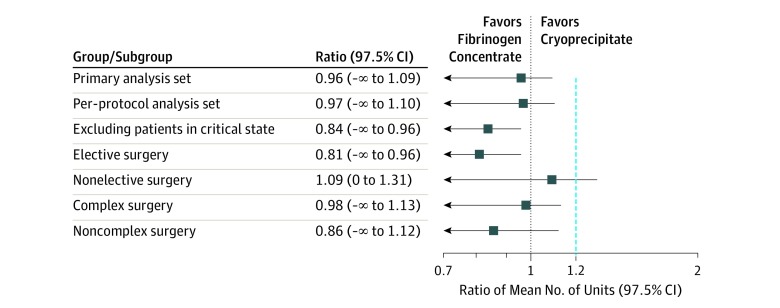
Main outcomes and measures: Primary outcome was blood components (red blood cells, platelets, plasma) administered during 24 hours post bypass. A 2-sample, 1-sided test for the ratio of the mean number of units was conducted to evaluate noninferiority (threshold for noninferiority ratio, <1.2).
Results: Of 827 randomized patients, 735 (372 fibrinogen concentrate, 363 cryoprecipitate) were treated and included in the primary analysis (median age, 64 [interquartile range, 53-72] years; 30% women; 72% underwent complex operations; 95% moderate to severe bleeding; and pretreatment fibrinogen level, 1.6 [interquartile range, 1.3-1.9] g/L). The trial met the a priori stopping criterion for noninferiority at the interim analysis after 827 of planned 1200 patients were randomized. Mean 24-hour postbypass allogeneic transfusions were 16.3 (95% CI, 14.9 to 17.8) units in the fibrinogen concentrate group and 17.0 (95% CI, 15.6 to 18.6) units in the cryoprecipitate group (ratio, 0.96 [1-sided 97.5% CI, -∞ to 1.09; P < .001 for noninferiority] [2-sided 95% CI, 0.84 to 1.09; P = .50 for superiority]). Thromboembolic events occurred in 26 patients (7.0%) in the fibrinogen concentrate group and 35 patients (9.6%) in the cryoprecipitate group.
Conclusions and relevance: In patients undergoing cardiac surgery who develop clinically significant bleeding and hypofibrinogenemia after cardiopulmonary bypass, fibrinogen concentrate is noninferior to cryoprecipitate with regard to number of blood components transfused in a 24-hour period post bypass. Use of fibrinogen concentrate may be considered for management of bleeding in patients with acquired hypofibrinogenemia in cardiac surgery.
Trial registration: ClinicalTrials.gov Identifier: NCT03037424.
Conflict of interest statement
Figures
Comment in
- doi: 10.1001/jama.2019.17313
References
-
- Boer C, Meesters MI, Milojevic M, et al. ; Task Force on Patient Blood Management for Adult Cardiac Surgery of the European Association for Cardio-Thoracic Surgery (EACTS) and the European Association of Cardiothoracic Anaesthesiology (EACTA) . 2017 EACTS/EACTA Guidelines on patient blood management for adult cardiac surgery. J Cardiothorac Vasc Anesth. 2018;32(1):88-120. doi:10.1053/j.jvca.2017.06.026 - DOI - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
