

Abnormalities of confidence in psychiatry: an overview and future perspectives
- PMID: 31636252
- PMCID: PMC6803712
- DOI: 10.1038/s41398-019-0602-7
Abnormalities of confidence in psychiatry: an overview and future perspectives
Abstract
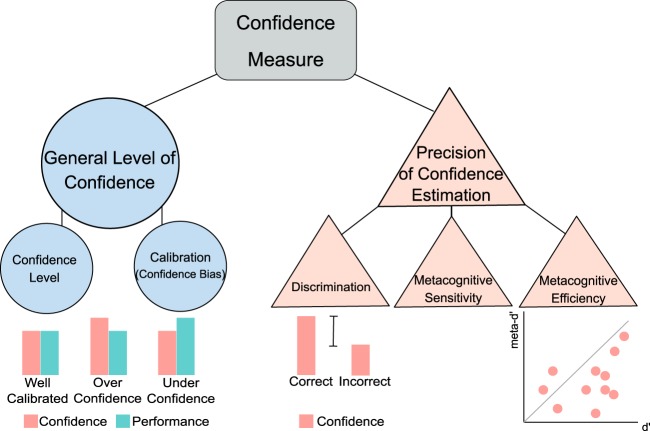
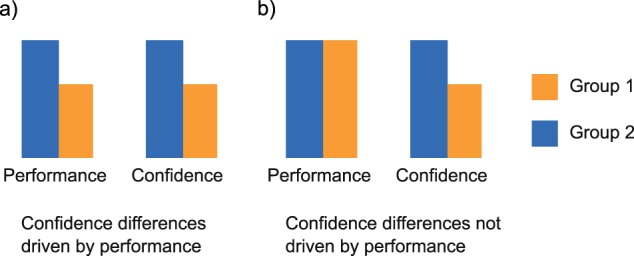
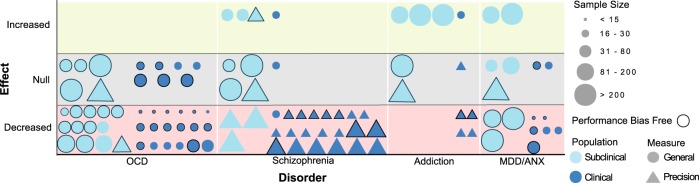
Our behavior is constantly accompanied by a sense of confidence and its' precision is critical for adequate adaptation and survival. Importantly, abnormal confidence judgments that do not reflect reality may play a crucial role in pathological decision-making typically seen in psychiatric disorders. In this review, we propose abnormalities of confidence as a new model of interpreting psychiatric symptoms. We hypothesize a dysfunction of confidence at the root of psychiatric symptoms either expressed subclinically in the general population or clinically in the patient population. Our review reveals a robust association between confidence abnormalities and psychiatric symptomatology. Confidence abnormalities are present in subclinical/prodromal phases of psychiatric disorders, show a positive relationship with symptom severity, and appear to normalize after recovery. In the reviewed literature, the strongest evidence was found for a decline in confidence in (sub)clinical OCD, and for a decrease in confidence discrimination in (sub)clinical schizophrenia. We found suggestive evidence for increased/decreased confidence in addiction and depression/anxiety, respectively. Confidence abnormalities may help to understand underlying psychopathological substrates across disorders, and should thus be considered transdiagnostically. This review provides clear evidence for confidence abnormalities in different psychiatric disorders, identifies current knowledge gaps and supplies suggestions for future avenues. As such, it may guide future translational research into the underlying processes governing these abnormalities, as well as future interventions to restore them.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
