

Nomogram to predict prolonged postoperative ileus after gastrectomy in gastric cancer
- PMID: 31636476
- PMCID: PMC6801185
- DOI: 10.3748/wjg.v25.i38.5838
Nomogram to predict prolonged postoperative ileus after gastrectomy in gastric cancer
Abstract
Background: Prolonged postoperative ileus (PPOI) is one of the common complications in gastric cancer patients who underwent gastrectomy. Evidence on the predictors of PPOI after gastrectomy is limited and few prediction models of nomogram are used to estimate the risk of PPOI. We hypothesized that a predictive nomogram can be used for clinical risk estimation of PPOI in gastric cancer patients.
Aim: To investigate the risk factors for PPOI and establish a nomogram for clinical risk estimation.
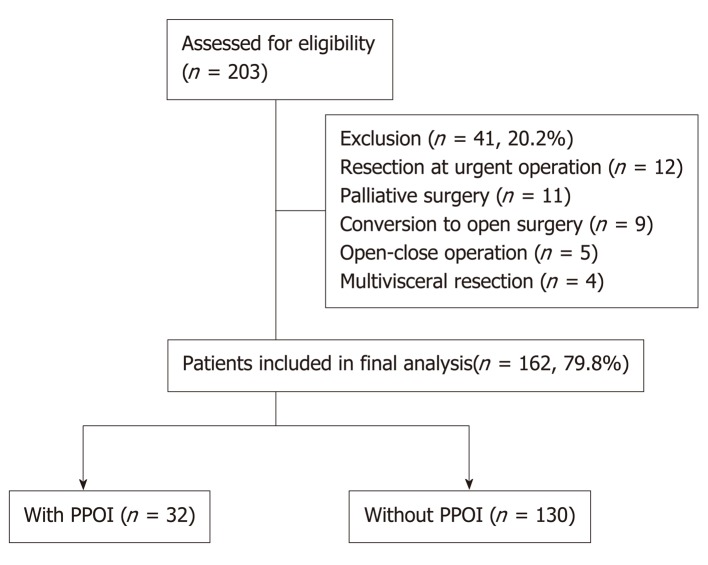
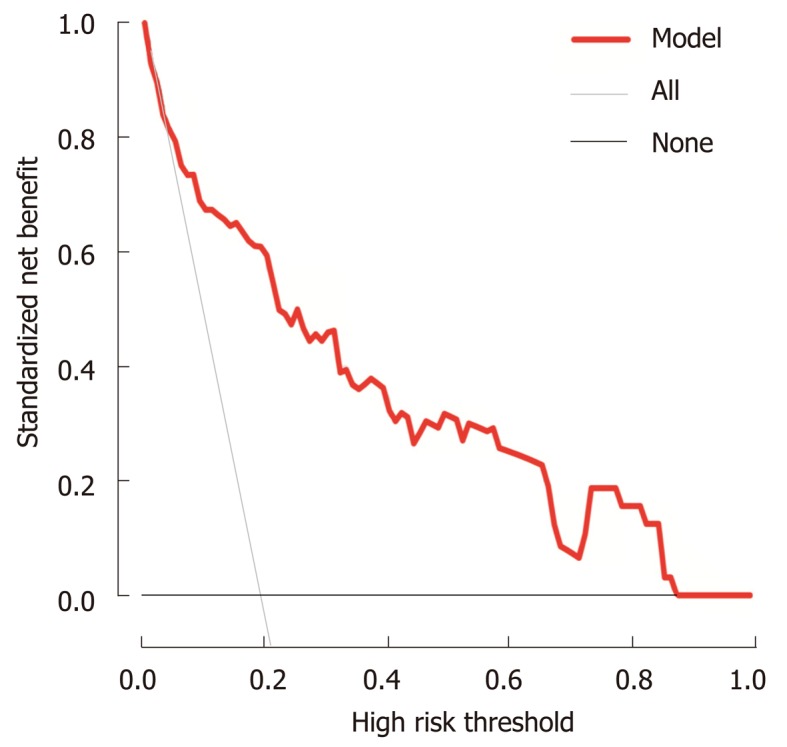
Methods: Between June 2016 and March 2017, the data of 162 patients with gastrectomy were obtained from a prospective and observational registry database. Clinical data of patients who fulfilled the criteria were obtained. Univariate and multivariable logistic regression models were performed to detect the relationship between variables and PPOI. A nomogram for PPOI was developed and verified by bootstrap resampling. The calibration curve was employed to detect the concentricity between the model probability curve and ideal curve. The clinical usefulness of our model was evaluated using the net benefit curve.
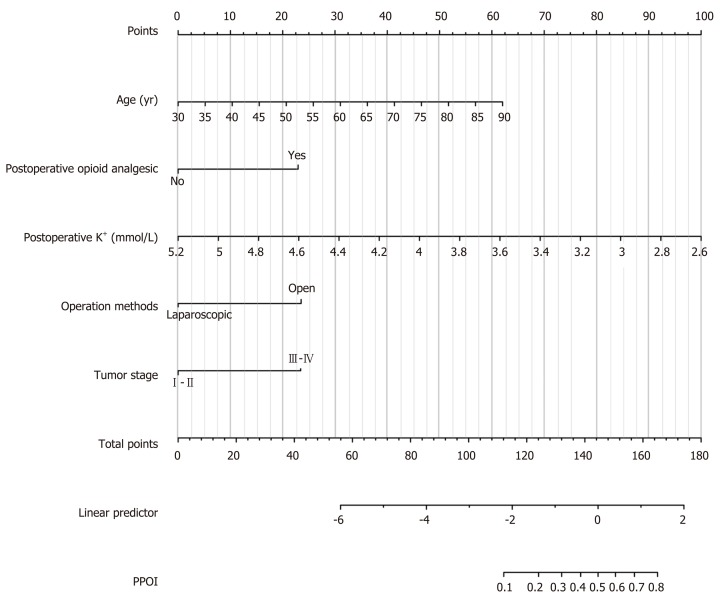
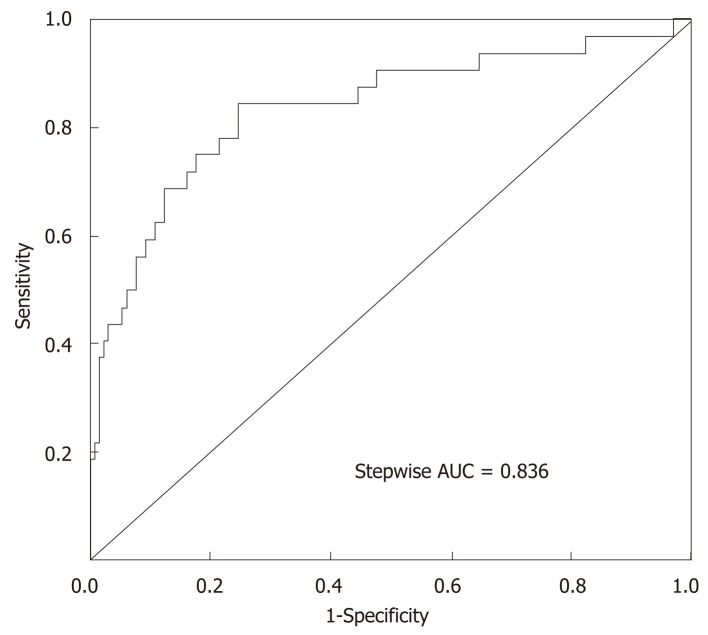
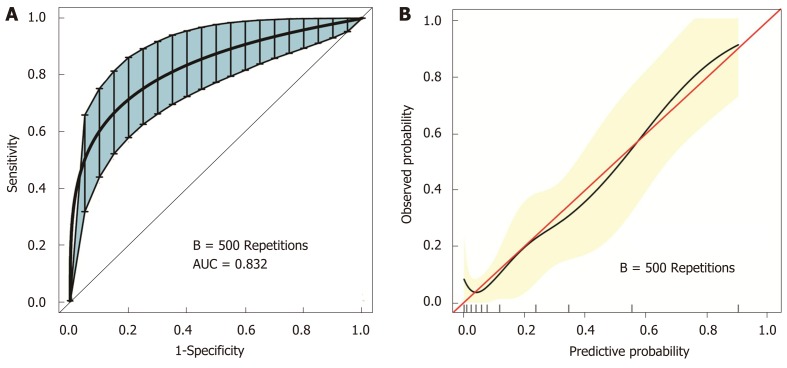
Results: This study analyzed 14 potential variables of PPOI in 162 gastric cancer patients who underwent gastrectomy. The incidence of PPOI was 19.75% in patients with gastrectomy. Age older than 60 years, open surgery, advanced stage (III-IV), and postoperative use of opioid analgesic were independent risk factors for PPOI. We developed a simple and easy-to-use prediction nomogram of PPOI after gastrectomy. This nomogram had an excellent diagnostic performance [area under the curve (AUC) = 0.836, sensitivity = 84.4%, and specificity = 75.4%]. This nomogram was further validated by bootstrapping for 500 repetitions. The AUC of the bootstrap model was 0.832 (95%CI: 0.741-0.924). This model showed a good fitting and calibration and positive net benefits in decision curve analysis.
Conclusion: We have developed a prediction nomogram of PPOI for gastric cancer. This novel nomogram might serve as an essential early warning sign of PPOI in gastric cancer patients.
Keywords: Bootstrap; Complication; Gastric cancer; Nomogram; Prolonged postoperative ileus.
©The Author(s) 2019. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: All the authors have no conflict of interest.
Figures
References
-
- van Bree SH, Nemethova A, Cailotto C, Gomez-Pinilla PJ, Matteoli G, Boeckxstaens GE. New therapeutic strategies for postoperative ileus. Nat Rev Gastroenterol Hepatol. 2012;9:675–683. - PubMed
-
- Pavoor R, Milsom J. Postoperative ileus after laparoscopic colectomy: elusive and expensive. Ann Surg. 2011;254:1075; author reply 1075–1075; author reply 1076. - PubMed
-
- Mowat AM. Janus-like monocytes regulate postoperative ileus. Gut. 2017;66:2049–2050. - PubMed
-
- van Bree SH, Bemelman WA, Hollmann MW, Zwinderman AH, Matteoli G, El Temna S, The FO, Vlug MS, Bennink RJ, Boeckxstaens GE. Identification of clinical outcome measures for recovery of gastrointestinal motility in postoperative ileus. Ann Surg. 2014;259:708–714. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
