

doi: 10.1093/eurheartj/ehz669.
Arrhythmogenic right ventricular cardiomyopathy: evaluation of the current diagnostic criteria and differential diagnosis
Collaborators,
Affiliations
- PMID: 31637441
- PMCID: PMC7138528
- DOI: 10.1093/eurheartj/ehz669
Item in Clipboard
Arrhythmogenic right ventricular cardiomyopathy: evaluation of the current diagnostic criteria and differential diagnosis
Eur Heart J.
.
No abstract available
Figures
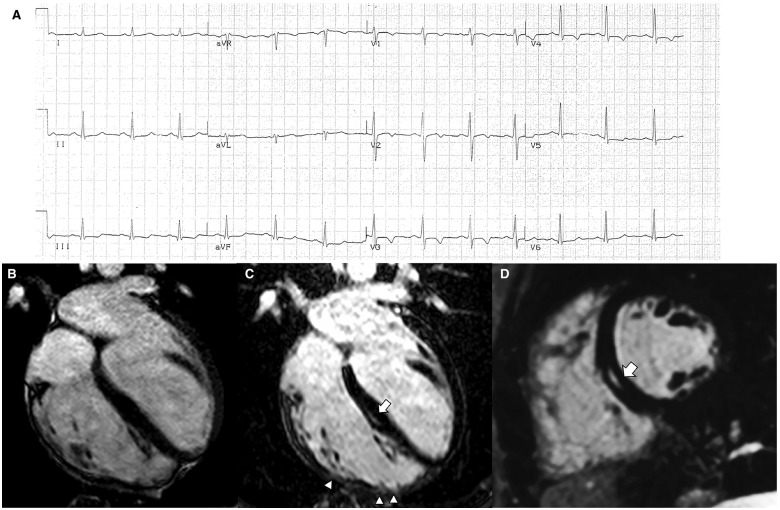
Electrocardiographic and cardiac magnetic resonance features of a representative case of right-dominant (classic) phenotypic variant of arrhythmogenic right ventricular cardiomyopathy. (A) Basal electrocardiographic showing T-wave inversion in right precordial leads (V1–V4). (B) End-diastolic frame of cine cardiac magnetic resonance sequence in long-axis four-chamber view showing a dilated right ventricle (end-diastolic volume, 127 mL/m2) with a severely reduced ejection fraction (25%). The post-contrast orthogonal images in long-axis (C) and short-axis (D) views show late gadolinium enhancement as mid-wall stria in the mid-septum (white arrow). In C, late gadolinium enhancement is also visible in the anterolateral, mid, and apical regions of the right ventricular wall, with segmental transmural involvement (white arrowheads) associated with regional dyskinesia (not shown). From De Lazzari et al.
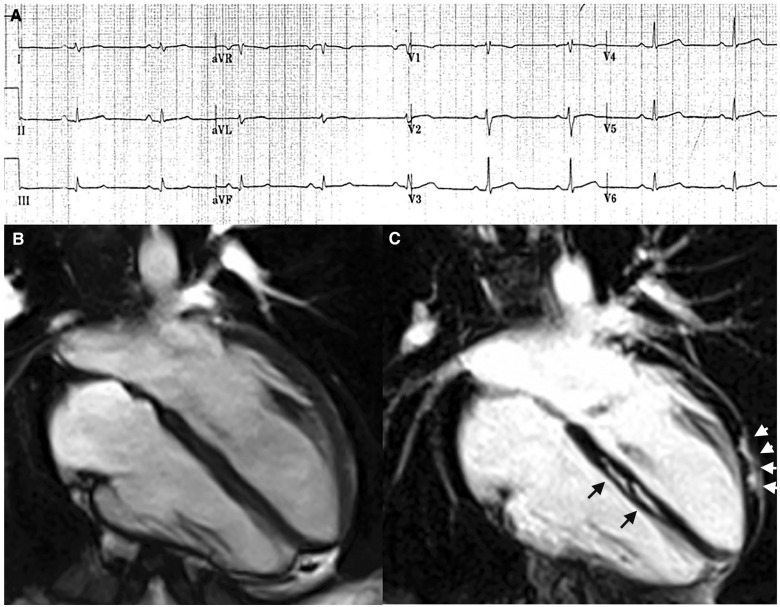
Electrocardiographic and cardiac magnetic resonance findings of a representative case of left-dominant phenotypic variant of arrhythmogenic right ventricular cardiomyopathy in a patient with a DSP-gene mutation and a history of sustained ventricular tachycardia. (A) Basal electrocardiographic showing low QRS voltages (<0.5 mV) in limb leads. (B) End-diastolic frame of cine cardiac magnetic resonance sequence in long-axis four-chamber view showing normal cavity size and function of both ventricles. (C) Post-contrast image showing myocardial fibrosis in the form of stria of late gadolinium enhancement in the epicardium of the left ventricular lateral wall (arrowheads) and mid-mural layer of the interventricular septum (arrows). From De Lazzari et al.
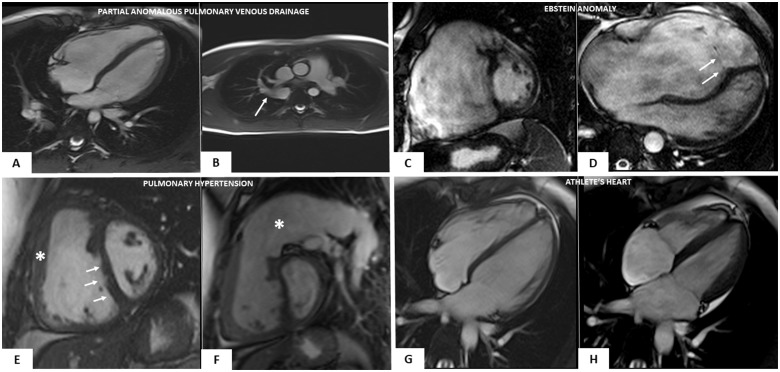
Cardiac magnetic resonance features of heart diseases mimicking right-dominant (classic) phenotypic variant of arrhythmogenic right ventricular cardiomyopathy. Partial anomalous pulmonary vein drainage (A and B): end-diastolic frame of cine cardiac magnetic resonance sequence in long-axis four-chamber view showing moderate right ventricular dilatation (A); cine sagittal view showing the anomalous drainage of the right pulmonary vein in the azygos vein (white arrow) (B). Ebstein anomaly (C and D): end-diastolic frame of cine cardiac magnetic resonance sequence in short-axis view showing a severe right ventricular enlargement due to a large ventricular ‘atrialization’ (C); end-diastolic frame of cine cardiac magnetic resonance sequence in four-chamber view showing a significant apical displacement of the septal leaflet of the tricuspid valve (white arrows) (D). Arterial pulmonary hypertension (E and F): end-diastolic frames of cine cardiac magnetic resonance sequence in short-axis view showing increase of the right ventricular wall thickness (white asterisk) (E), flattening of the interventricular septum (white arrows) (E), and massive pulmonary artery dilatation (white asterisk) (F). Athlete’s heart (G and H): end-diastolic (G) and systolic (H) frames of cine cardiac magnetic resonance sequence in four-chamber view evidencing biventricular dilatation (end-diastolic volume 122 mL/m2) and normal systolic function (ejection fraction 64%), in the absence of wall motion abnormalities (not shown).
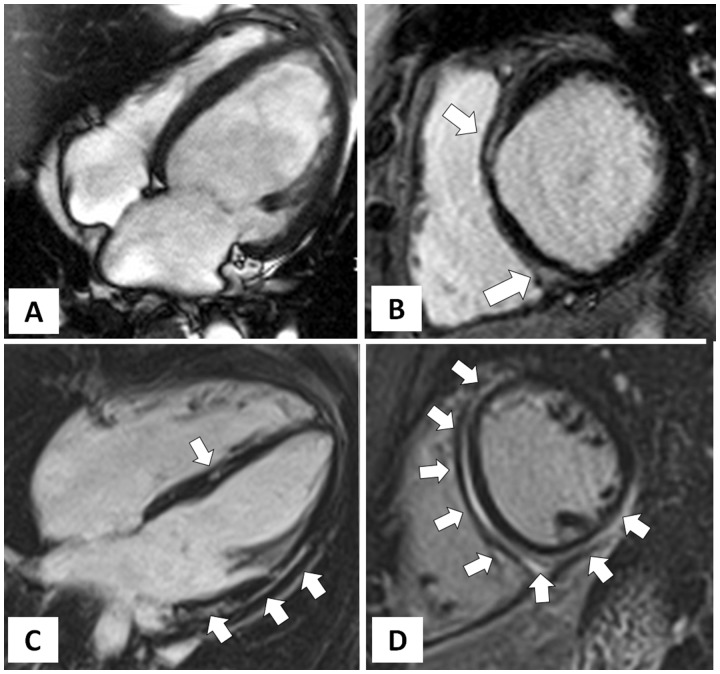
Cardiac magnetic resonance features of dilated cardiomyopathy vs. left-dominant phenotypic variant of arrhythmogenic right ventricular cardiomyopathy. Dilated cardiomyopathy (A and B): end-diastolic frame of cine cardiac magnetic resonance sequence in four-chamber view showing severe left ventricular dilatation (A) with severe systolic dysfunction (not shown); post-contrast T1 inversion recovery sequence in short-axis view showing limited mid-wall late gadolinium enhancement in the anterior interventricular septum and infero-septal junction involving the adjacent infero-basal wall (white arrow) (B). Left-dominant arrhythmogenic right ventricular cardiomyopathy (C and D): post-contrast T1 inversion recovery sequence in four-chamber view showing a non-dilated (C) and hypokinetic (not shown) left ventricle; post-contrast T1 inversion recovery sequence in short-axis view showing a large amount of late gadolinium enhancement involving the interventricular septum and both anterior and inferolateral left ventricular walls (C and D).
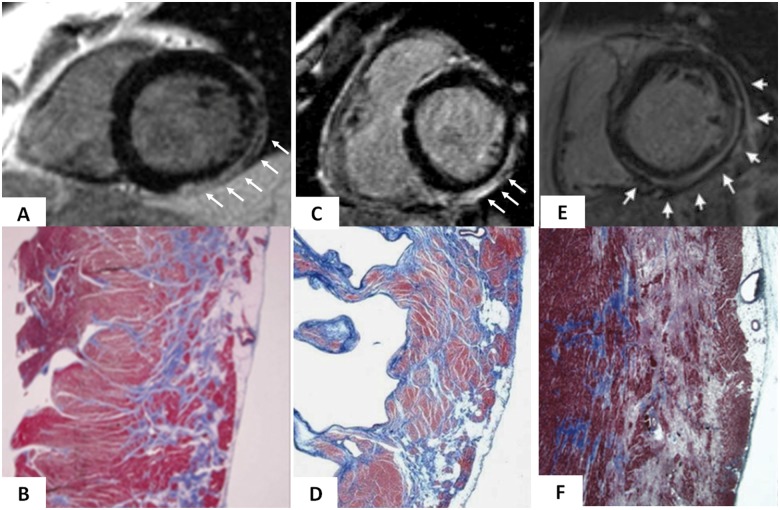
Cardiac magnetic resonance features and histopathologic findings of non-ischaemic left ventricular scar of different aetiologies. Muscular dystrophy (A and B): post-contrast T1 inversion recovery sequence in short-axis view showing a subepicardial stria of late gadolinium enhancement in the left ventricular wall (white arrows) (A); corresponding panoramic histopathologic view of the inferolateral left ventricular wall showing replacement-type fibrosis confined to the outer-mid layer of the musculature (B). Modified from Yilmaz et al. Chronic myocarditis (C and D): post-contrast T1 inversion recovery sequence in short-axis view showing subepicardial late gadolinium enhancement of the inferolateral left ventricular wall (C); corresponding panoramic histopathologic view of the inferolateral left ventricular wall showing extensive fibrous tissue replacement in the subepicardial layer of the musculature (D). From Yilmaz et al. Desmosomal gene-related, left-sided arrhythmogenic right ventricular cardiomyopathy (E and F): post-contrast T1 inversion recovery sequence in short-axis view showing subepicardial late gadolinium enhancement of the infero-lateral left ventricular wall in a DSP-gene mutation carrier (E). Panoramic histopathologic view showing myocardial replacement of the outer layer of the infero-lateral left ventricular wall in a sudden cardiac death victim carrying a DSP-gene mutation (F). From Zorzi et al.
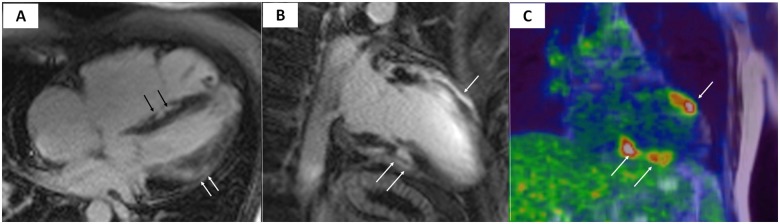
Magnetic resonance and cardiac positron emission tomography features of cardiac sarcoidosis. Post-contrast T1 inversion recovery sequence in four-chamber view showing right ventricular dilatation and late gadolinium enhancement of the interventricular septum (black arrows) and subepicardial lateral left ventricular wall (white arrows) (A). Topographic concordance between the epicardial spot of late gadolinium enhancement involving the anterior (B, single white arrow) and inferior (B, white arrows) left ventricular regions and the areas of fludeoxyglucose uptake on positron emission tomography (C, white arrows pointing to yellow–red areas).
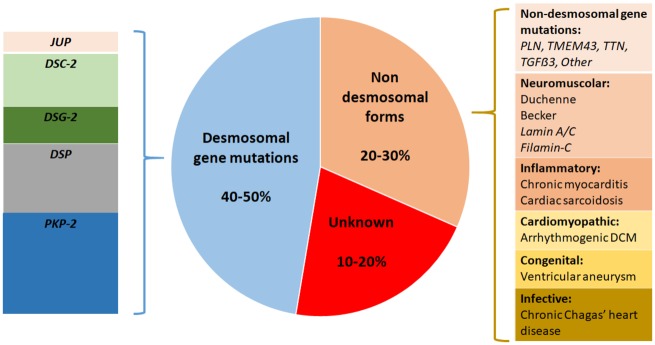
Aetiologic classification of arrhythmogenic cardiomyopathies. The most common cause of arrhythmogenic cardiomyopathy is a genetic defect of desmosomal genes, although there are other genetic and non-genetic causes (see the text for details).
Comment in
-
Cardiovascular magnetic resonance imaging volume criteria for arrhythmogenic right ventricular cardiomyopathy: need for update?Eur Heart J. 2020 Apr 7;41(14):1451. doi: 10.1093/eurheartj/ehz965. Eur Heart J. 2020. PMID: 32031606 No abstract available.
-
Right ventricular dilatation in arrhythmogenic right ventricular cardiomyopathy: need for a revision of the 2010 International Task Force criteria.Eur Heart J. 2020 Apr 7;41(14):1452-1453. doi: 10.1093/eurheartj/ehaa003. Eur Heart J. 2020. PMID: 32031609 No abstract available.
References
-
- Thiene G, Nava A, Corrado D, Rossi L, Pennelli N.. Right ventricular cardiomyopathy and sudden death in young people. N Engl J Med 1988;318:129–133. - PubMed
-
- Corrado D, Link MS, Calkins H.. Arrhythmogenic right ventricular cardiomyopathy. N Engl J Med 2017;376:61–72. - PubMed
-
- Corrado D, Basso C, Judge DP.. Arrhythmogenic cardiomyopathy. Circ Res 2017;121:784–802. - PubMed
-
- Basso C, Thiene G, Corrado D, Angelini A, Nava A, Valente M.. Arrhythmogenic right ventricular cardiomyopathy. Dysplasia, dystrophy, or myocarditis? Circulation 1996;94:983–991. - PubMed
-
- Corrado D, Basso C, Thiene G, McKenna WJ, Davies MJ, Fontaliran F, Nava A, Silvestri F, Blomstrom-Lundqvist C, Wlodarska EK, Fontaine G, Camerini F.. Spectrum of clinicopathologic manifestations of arrhythmogenic right ventricular cardiomyopathy/dysplasia: a multicenter study. J Am Coll Cardiol 1997;30:1512–1520. - PubMed
