

Bone Flap Changes after Cranioplasty Using Frozen Autologous Bone Flaps: A Three-Dimensional Volumetric Reconstruction Study
- PMID: 31637889
- PMCID: PMC6813147
- DOI: 10.3349/ymj.2019.60.11.1067
Bone Flap Changes after Cranioplasty Using Frozen Autologous Bone Flaps: A Three-Dimensional Volumetric Reconstruction Study
Erratum in
-
Erratum to "Bone Flap Changes after Cranioplasty Using Frozen Autologous Bone Flaps: A Three-Dimensional Volumetric Reconstruction Study" by Lee JH, et al. (Yonsei Med J 2019 Nov;60(11):1067-1073).Yonsei Med J. 2023 Dec;64(12):750. doi: 10.3349/ymj.2019.0141.er. Yonsei Med J. 2023. PMID: 37992748 Free PMC article.
Abstract
Purpose: Bone flap resorption (BFR) after cranioplasty with an autologous bone flap (ABF) is well known. However, the prevalences and degrees of BFR remain unclear. This study aimed to evaluate changes in ABFs following cranioplasty and to investigate factors related with BFR.
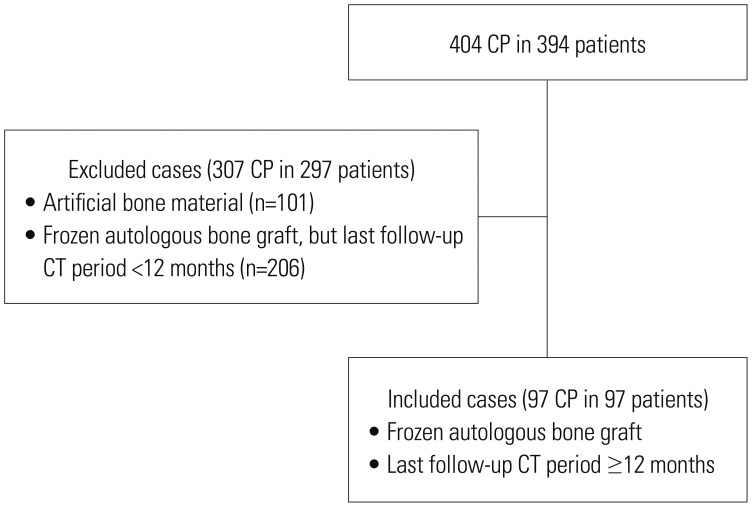
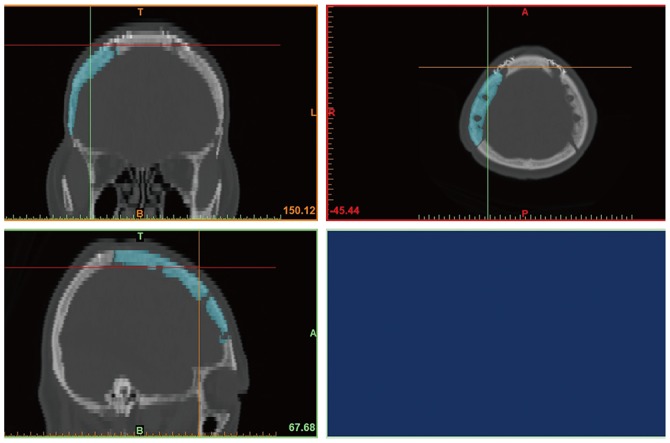
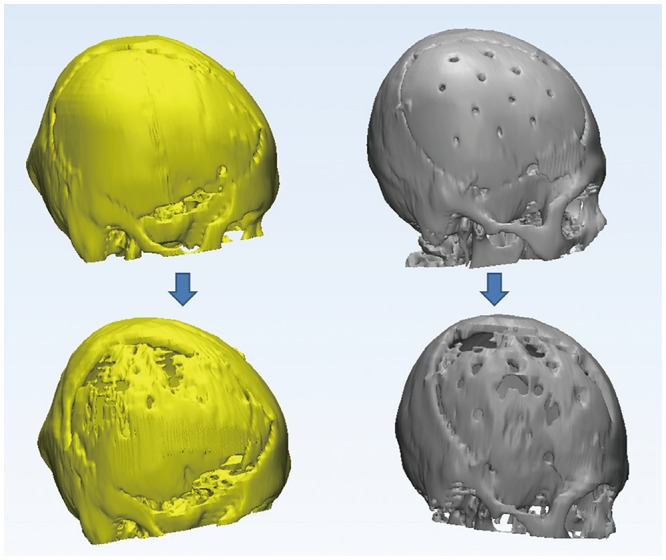
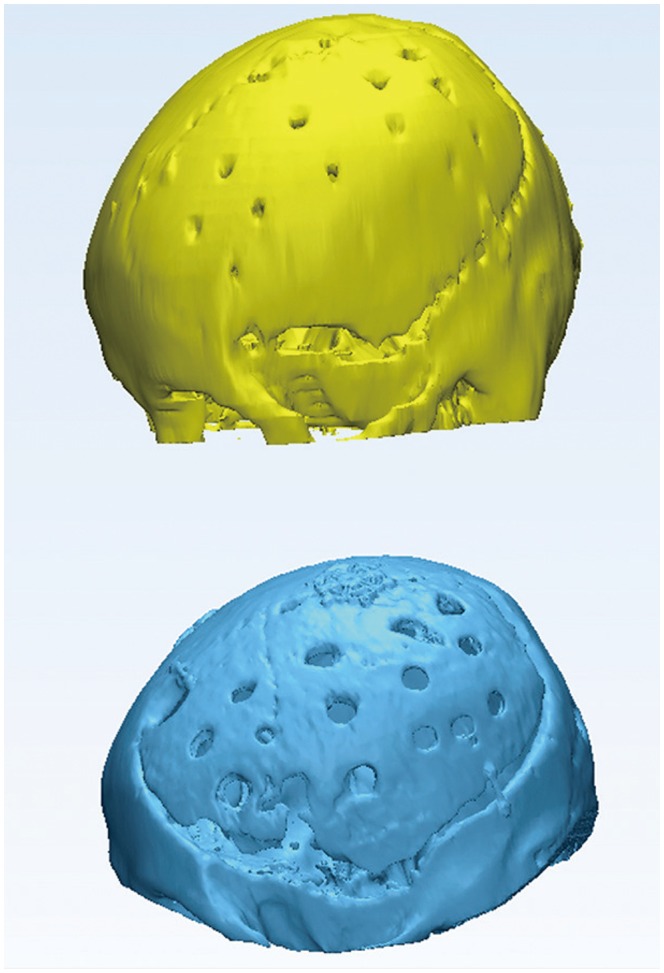
Materials and methods: We retrospectively reviewed 97 patients who underwent cranioplasty with frozen ABF between January 2007 and December 2016. Brain CT images of these patients were reconstructed to form three-dimensional (3D) images, and 3D images of ABF were separated using medical image editing software. ABF volumes on images were measured using 3D image editing software and were compared between images in the immediate postoperative period and at postoperative 12 months. Risk factors related with BFR were also analyzed.
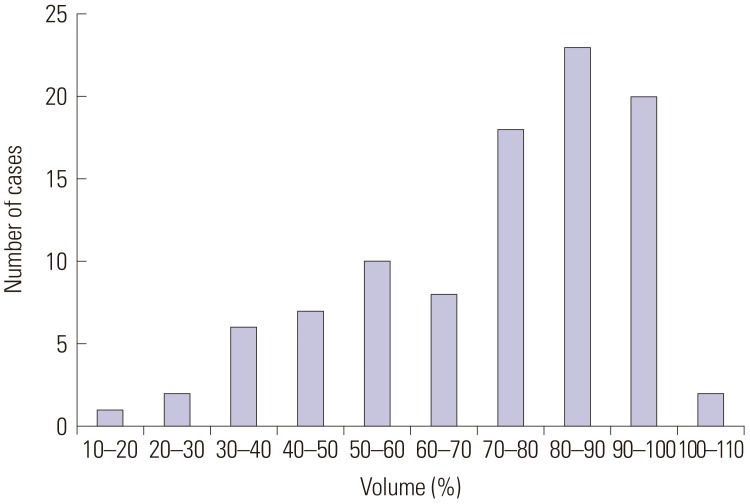
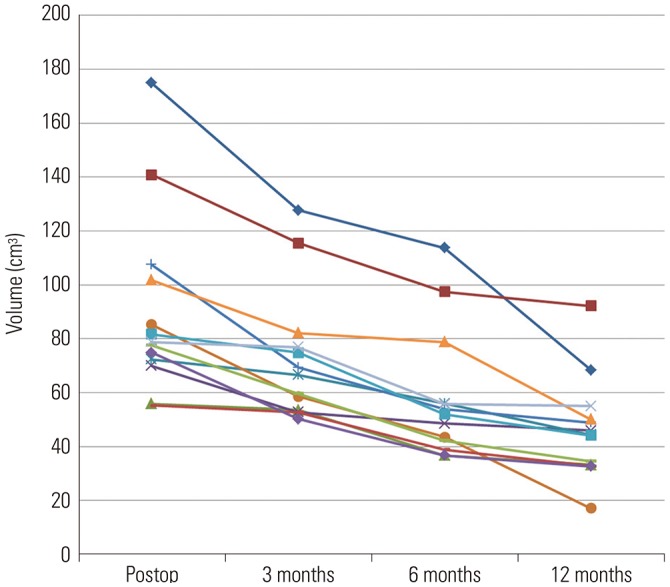
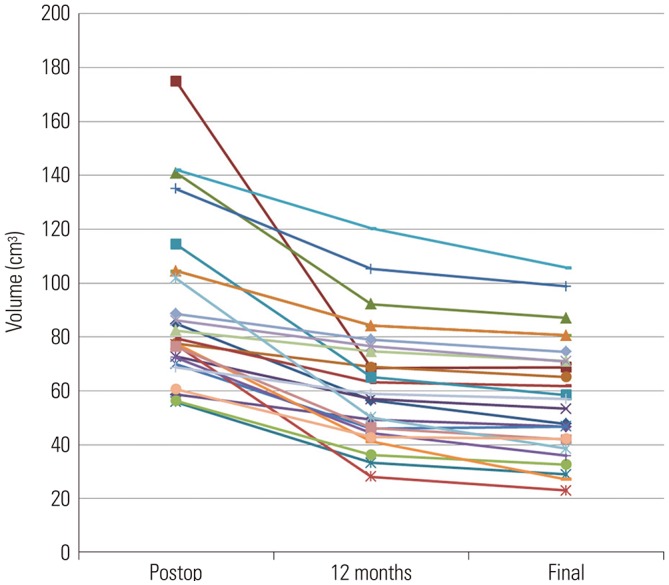
Results: The volumes of bone flaps calculated from CT images immediately after cranioplasty ranged from 55.3 cm³ to 175 cm³. Remnant bone flap volumes at postoperative 12 months ranged from 14.2% to 102.5% of the original volume. Seventy-five patients (77.3%) had a BFR rate exceeding 10% at 12 months after cranioplasty, and 26 patients (26.8%) presented severe BFR over 40%. Ten patients (10.3%) underwent repeated cranioplasty due to severe BFR. The use of a 5-mm burr for central tack-up sutures was significantly associated with BFR (p<0.001).
Conclusion: Most ABFs after cranioplasty are absorbed. Thus, when using frozen ABF, patients should be adequately informed. To prevent BFR, making holes must be kept to a minimum during ABF grafting.
Keywords: Autografts; bone resorption; cranioplasty; decompressive craniectomy; skull.
© Copyright: Yonsei University College of Medicine 2019.
Conflict of interest statement
The authors have no potential conflicts of interest to disclose.
Figures
References
-
- Hofmeijer J, Kappelle LJ, Algra A, Amelink GJ, van Gijn J, van der Worp HB HAMLET investigators. Surgical decompression for space-occupying cerebral infarction (the Hemicraniectomy After Middle Cerebral Artery infarction with Life-threatening Edema Trial [HAMLET]): a multicentre, open, randomised trial. Lancet Neurol. 2009;8:326–333. - PubMed
-
- Fisher CM, Ojemann RG. Bilateral decompressive craniectomy for worsening coma in acute subarachnoid hemorrhage. Observations in support of the procedure. Surg Neurol. 1994;41:65–74. - PubMed
-
- Guerra WK, Gaab MR, Dietz H, Mueller JU, Piek J, Fritsch MJ. Surgical decompression for traumatic brain swelling: indications and results. J Neurosurg. 1999;90:187–196. - PubMed
-
- Honeybul S, Ho KM. How “successful” is calvarial reconstruction using frozen autologous bone? Plast Reconstr Surg. 2012;130:1110–1117. - PubMed
-
- Dujovny M, Fernandez P, Alperin N, Betz W, Misra M, Mafee M. Post-cranioplasty cerebrospinal fluid hydrodynamic changes: magnetic resonance imaging quantitative analysis. Neurol Res. 1997;19:311–316. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
