

Prevalence of Survival Without Major Comorbidities Among Adults Born Prematurely
- PMID: 31638681
- PMCID: PMC6806441
- DOI: 10.1001/jama.2019.15040
Prevalence of Survival Without Major Comorbidities Among Adults Born Prematurely
Abstract
Importance: Preterm birth has been associated with cardiometabolic, respiratory, and neuropsychiatric disorders in adulthood. However, the prevalence of survival without any major comorbidities is unknown.
Objective: To determine the prevalence of survival without major comorbidities in adulthood among persons born preterm vs full-term.
Design, setting, and participants: National cohort study of all 2 566 699 persons born in Sweden from January 1, 1973, through December 31, 1997, who had gestational age data and who were followed up for survival and comorbidities through December 31, 2015 (ages 18-43 years).
Exposures: Gestational age at birth.
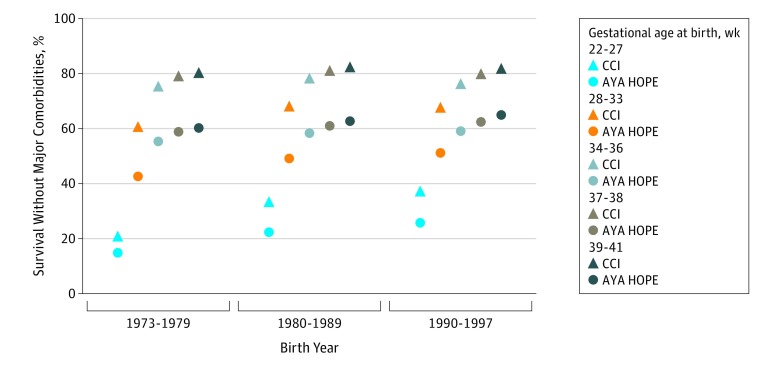
Main outcomes and measures: Survival without major comorbidities among persons born extremely preterm (22-27 weeks), very preterm (28-33 weeks), late preterm (34-36 weeks), or early term (37-38 weeks), compared with full-term (39-41 weeks). Comorbidities were defined using the Adolescent and Young Adult Health Outcomes and Patient Experience (AYA HOPE) Comorbidity Index, which includes conditions that commonly manifest in adolescence or young adulthood, including neuropsychiatric disorders; and the Charlson Comorbidity Index (CCI), which includes major chronic disorders predictive of mortality in adulthood. Poisson regression was used to determine prevalence ratios and differences, adjusted for potential confounders.
Results: In this study population, 48.6% were female, 5.8% were born preterm, and the median age at end of follow-up was 29.8 years (interquartile range, 12.6 years). Of all persons born preterm, 54.6% were alive with no AYA HOPE comorbidities at the end of follow-up. Further stratified, this prevalence was 22.3% for those born extremely preterm, 48.5% for very preterm, 58.0% for late preterm, 61.2% for early term, and 63.0% for full-term. These prevalences were significantly lower for earlier gestational ages vs full-term (eg, adjusted prevalence ratios: extremely preterm, 0.35 [95% CI, 0.33 to 0.36; P < .001]; all preterm, 0.86 [95% CI, 0.85 to 0.86; P < .001]; adjusted prevalence differences: extremely preterm, -0.41 [95% CI, -0.42 to -0.40; P < .001]; all preterm, -0.09 [95% CI, -0.09 to -0.09; P < .001]). Using the CCI, the corresponding prevalences were 73.1% (all preterm), 32.5% (extremely preterm), 66.4% (very preterm), 77.1% (late preterm), 80.4% (early term), and 81.8% (full-term) (adjusted prevalence ratios: extremely preterm, 0.39 [95% CI, 0.38 to 0.41; P < .001]; all preterm, 0.89 [95% CI, 0.89 to 0.89; P < .001]; adjusted prevalence differences: extremely preterm, -0.50 [95% CI, -0.51 to -0.49; P < .001]; all preterm, -0.09 [95% CI, -0.09 to -0.09; P < .001]).
Conclusions and relevance: Among persons born preterm in Sweden between 1973 and 1997, the majority survived to early to mid-adulthood without major comorbidities. However, outcomes were worse for those born extremely preterm.
Conflict of interest statement
Figures
Comment in
-
Most babies born preterm survive into adulthood without comorbidities.J Pediatr. 2020 Mar;218:259-262. doi: 10.1016/j.jpeds.2019.12.048. J Pediatr. 2020. PMID: 32089181 No abstract available.
References
-
- Raju TNK, Pemberton VL, Saigal S, Blaisdell CJ, Moxey-Mims M, Buist S; Adults Born Preterm Conference Speakers and Discussants . Long-term healthcare outcomes of preterm birth: an executive summary of a conference sponsored by the National Institutes of Health. J Pediatr. 2017;181:309-318. doi:10.1016/j.jpeds.2016.10.015 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
