

Microbial biofilm correlates with an increased antibiotic tolerance and poor therapeutic outcome in infective endocarditis
- PMID: 31638894
- PMCID: PMC6802308
- DOI: 10.1186/s12866-019-1596-2
Microbial biofilm correlates with an increased antibiotic tolerance and poor therapeutic outcome in infective endocarditis
Abstract
Background: Infective endocarditis (IE) is associated with high rates of mortality. Prolonged treatments with high-dose intravenous antibiotics often fail to eradicate the infection, frequently leading to high-risk surgical intervention. By providing a mechanism of antibiotic tolerance, which escapes conventional antibiotic susceptibility profiling, microbial biofilm represents a key diagnostic and therapeutic challenge for clinicians. This study aims at assessing a rapid biofilm identification assay and a targeted antimicrobial susceptibility profile of biofilm-growing bacteria in patients with IE, which were unresponsive to antibiotic therapy.
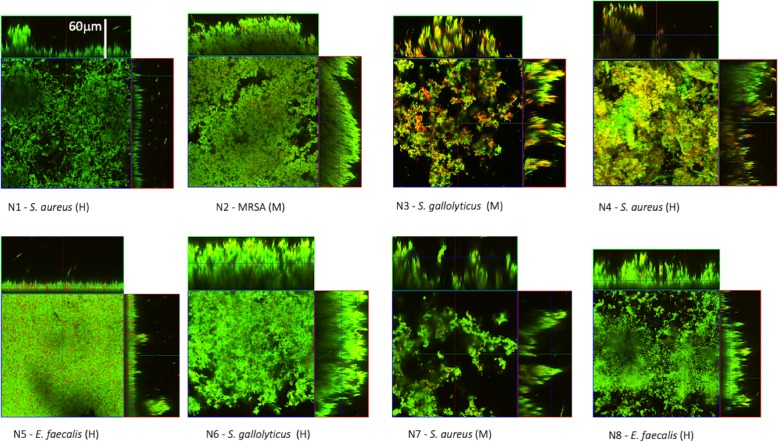
Results: Staphylococcus aureus was the most common isolate (50%), followed by Enterococcus faecalis (25%) and Streptococcus gallolyticus (25%). All microbial isolates were found to be capable of producing large, structured biofilms in vitro. As expected, antibiotic treatment either administered on the basis of antibiogram or chosen empirically among those considered first-line antibiotics for IE, including ceftriaxone, daptomycin, tigecycline and vancomycin, was not effective at eradicating biofilm-growing bacteria. Conversely, antimicrobial susceptibility profile of biofilm-growing bacteria indicated that teicoplanin, oxacillin and fusidic acid were most effective against S. aureus biofilm, while ampicillin was the most active against S. gallolyticus and E. faecalis biofilm, respectively.
Conclusions: This study indicates that biofilm-producing bacteria, from surgically treated IE, display a high tolerance to antibiotics, which is undetected by conventional antibiograms. The rapid identification and antimicrobial tolerance profiling of biofilm-growing bacteria in IE can provide key information for both antimicrobial therapy and prevention strategies.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Pant S, Patel NJ, Deshmukh A, Golwala H, Patel N, Badheka A, Hirsch GA, Mehta JL. Trends in infective endocarditis incidence, microbiology, and valve replacement in the United States from 2000 to 2011. J Am Coll Cardiol. 2015;65:2070–2076. - PubMed
-
- Baddour LM, Wilson WR, Bayer AS, Fowler VG, Jr, Tleyjeh IM, Rybak MJ, et al. Infective endocarditis in adults: diagnosis, antimicrobial therapy, and management of complications: a scientific statement for healthcare professionals from the American Heart Association. Circulation. 2015;132:1435–1486. - PubMed
-
- Gatti G, Benussi B, Gripshi F, Della Mattia A, Proclemer A, Cannatà A, et al. A risk factor analysis for in-hospital mortality after surgery for infective endocarditis and a proposal of a new predictive scoring system. Infection. 2017;45:413–423. - PubMed
-
- Østergaard L, Valeur N, Wang A, Bundgaard H, Aslam M, Gislason G, et al. Incidence of infective endocarditis in patients considered at moderate risk. Eur Heart J. 2018. 10.1093/eurheartj/ehy629. - PubMed
-
- Murdoch DR, Corey GR, Hoen B, Miró JM, Fowler VG, Jr, Bayer AS, et al. International collaboration on endocarditis-prospective cohort study (ICE-PCS) investigators. 2009. Clinical presentation, etiology, and outcome of infective endocarditis in the 21st century: the international collaboration on endocarditis-prospective cohort study. Arch Intern Med. 2009;169:463–473. - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
