

Plasmacytoid urothelial carcinoma: a rapid autopsy case report with unique clinicopathologic and genomic profile
- PMID: 31638990
- PMCID: PMC6802321
- DOI: 10.1186/s13000-019-0896-z
Plasmacytoid urothelial carcinoma: a rapid autopsy case report with unique clinicopathologic and genomic profile
Abstract
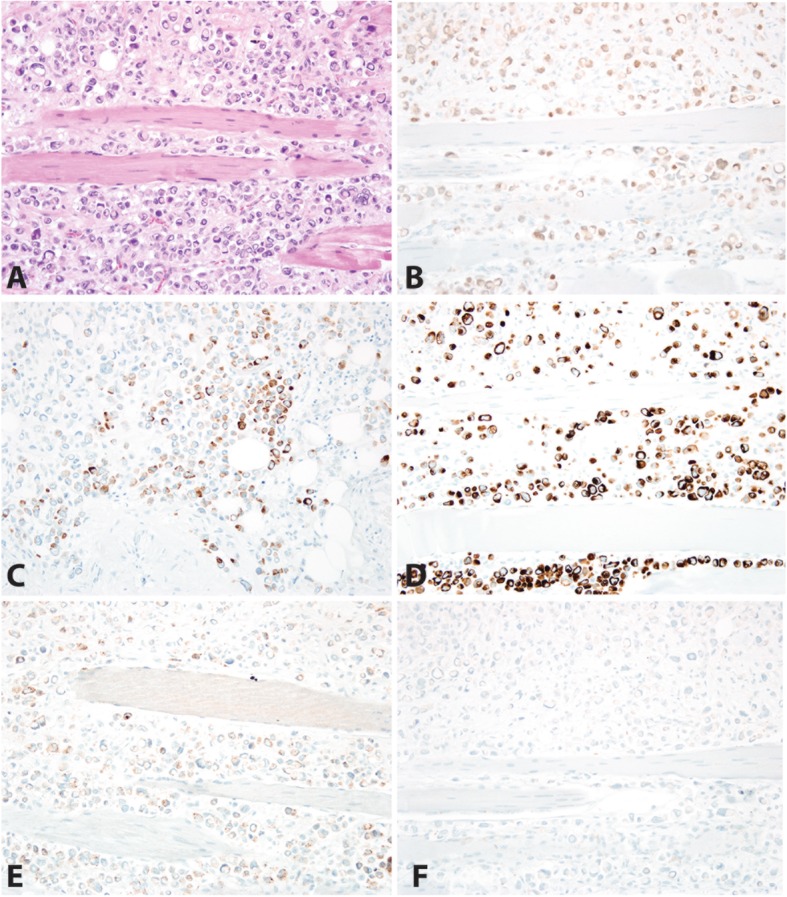
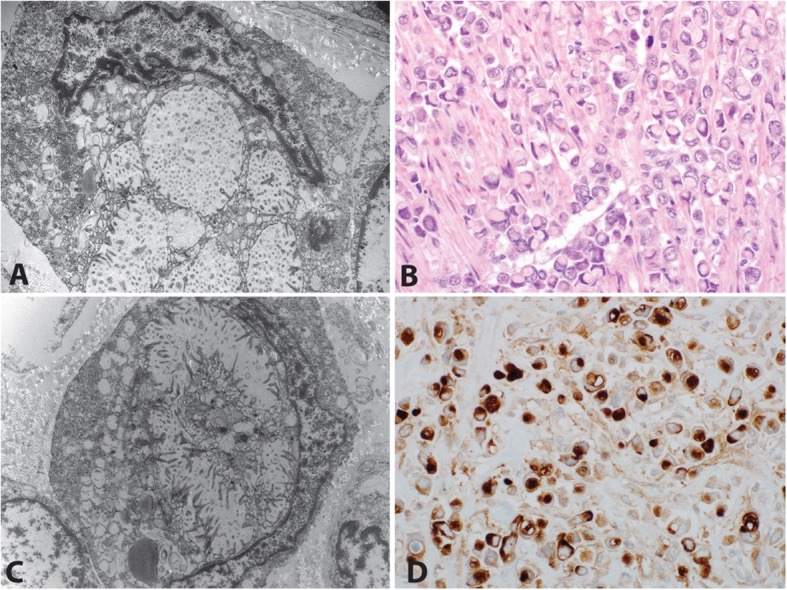
Background: Rapid ("warm") autopsies of patients with advanced metastatic cancer provide important insight into the natural history, pathobiology and histomorphology of disease in treatment-resistant tumors. Plasmacytoid urothelial carcinoma (PUC) is a rare variant of urothelial carcinoma characterized by neoplastic cells morphologically resembling plasma cells. PUC is typically aggressive, high-stage at presentation, and associated with poor outcomes. Recurrence is common in PUC, with the majority of recurrences occurring in the peritoneum.
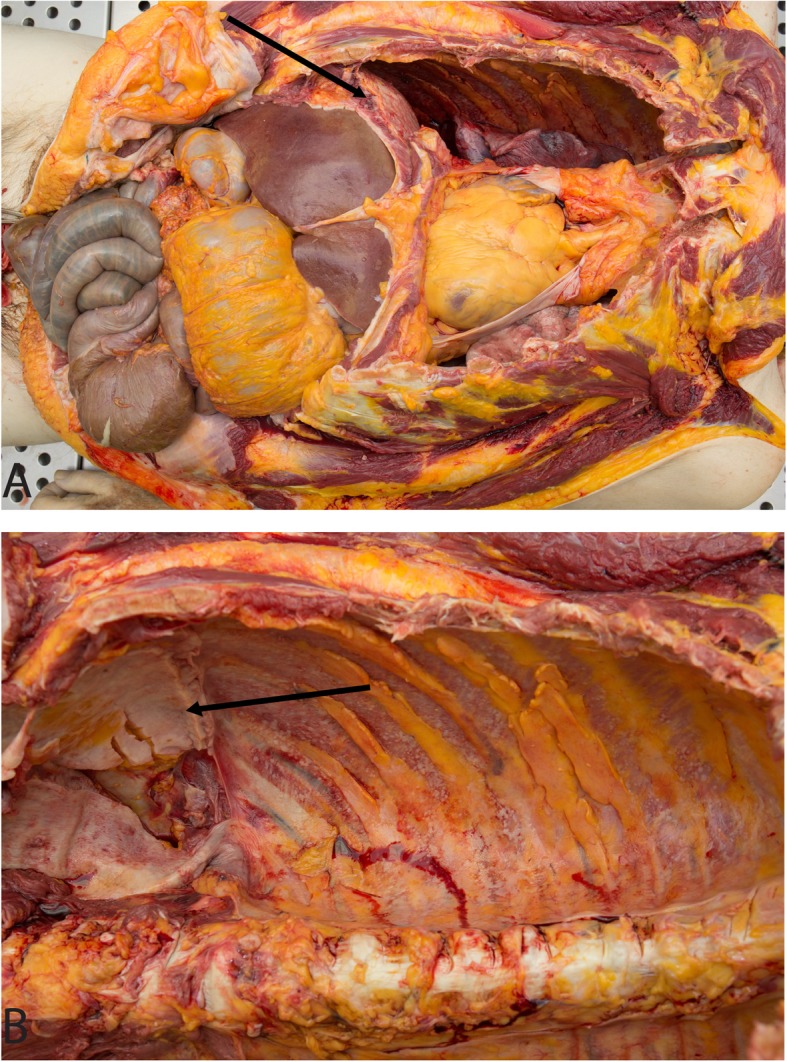
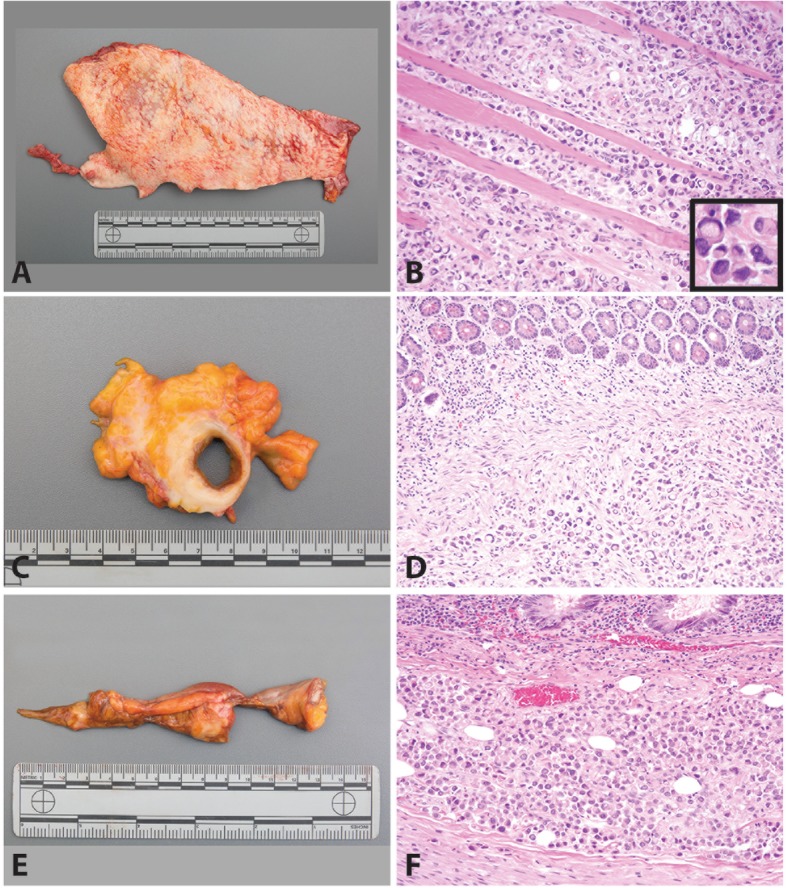
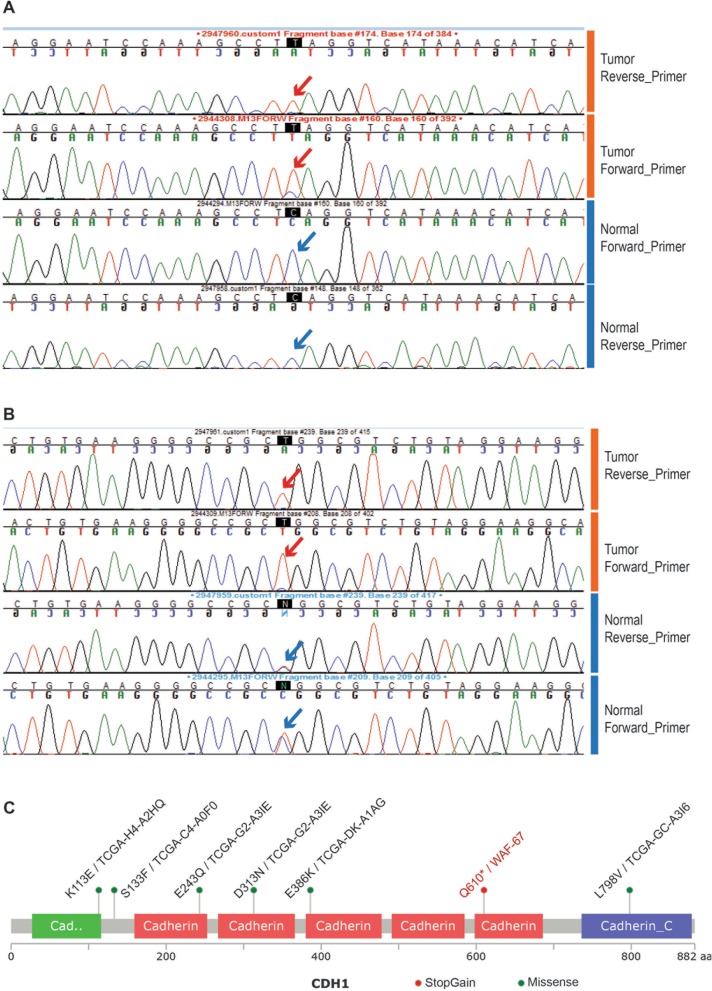
Case presentation: Here, we report rapid autopsy findings from a patient with recurrent PUC. The patient had persistent pain after cystoprostatectomy, although initial post-operative imaging showed no evidence of disease. Imaging obtained shortly before his death showed only subtle growth along vascular tissue planes; however, extensive disease was seen on autopsy. Plasmacytoid tumor cells formed sheets involving many serosal surfaces. Molecular interrogation confirmed a mutation in CDH1 exon 12 leading to early truncation of the CDH1 protein in the tumor cells.
Conclusions: The sheet-like growth pattern of PUC makes early phases of disease spread much more difficult to capture on cross-sectional imaging. Alternative forms of surveillance may be required for detection of recurrent PUC, and providers may need to treat based on symptoms and clinical suspicion.
Keywords: CDH1; Plasmacytoid; Rapid autopsy; Urothelial carcinoma.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Rubin MA, Putzi M, Mucci N, et al. Rapid (“warm”) autopsy study for procurement of metastatic prostate cancer. Clin Cancer Res. 2000;6:138–1038-1045. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
