

Clinical and Laboratory Predictors for Plaque Erosion in Patients With Acute Coronary Syndromes
- PMID: 31640466
- PMCID: PMC6898801
- DOI: 10.1161/JAHA.119.012322
Clinical and Laboratory Predictors for Plaque Erosion in Patients With Acute Coronary Syndromes
Abstract
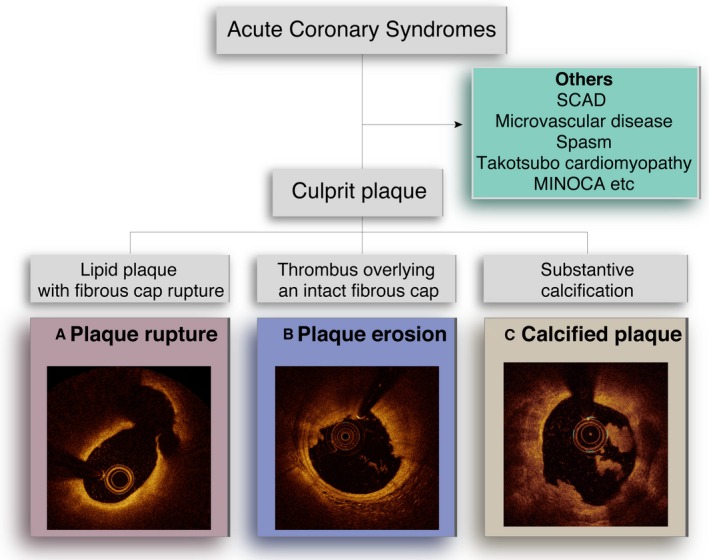
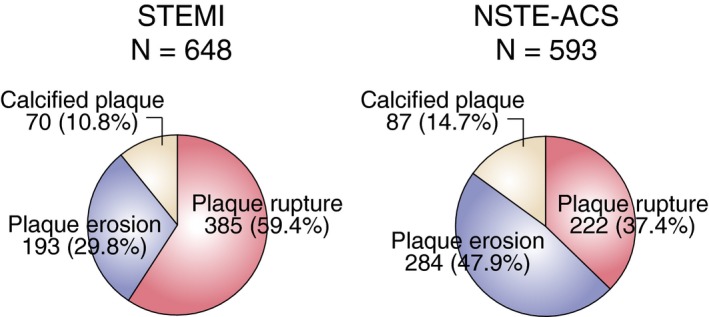
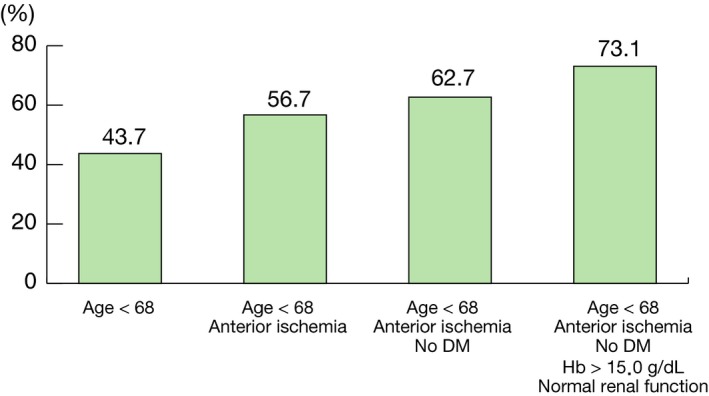
Background Plaque erosion is responsible for 25% to 40% of patients with acute coronary syndromes (ACS). Recent studies suggest that anti-thrombotic therapy without stenting may be an option for this subset of patients. Currently, however, an invasive procedure is required to make a diagnosis of plaque erosion. The aim of this study was to identify clinical or laboratory predictors of plaque erosion in patients with ACS to enable a diagnosis of erosion without additional invasive procedures. Methods and Results Patients with ACS who underwent optical coherence tomography imaging were selected from 11 institutions in 6 countries. The patients were classified into plaque rupture, plaque erosion, or calcified plaque, and predictors were identified using multivariable logistic modeling. Among 1241 patients with ACS, 477 (38.4%) patients were found to have plaque erosion. Plaque erosion was more frequent in non-ST-segment elevation-ACS than in ST-segment-elevation myocardial infarction (47.9% versus 29.8%, P=0.0002). Multivariable logistic regression models showed 5 independent parameters associated with plaque erosion: age <68 years, anterior ischemia, no diabetes mellitus, hemoglobin >15.0 g/dL, and normal renal function. When all 5 parameters are present in a patient with non-ST-segment elevation-ACS, the probability of plaque erosion increased to 73.1%. Conclusions Clinical and laboratory parameters associated with plaque erosion are explored in this retrospective registry study. These parameters may be useful to identify the subset of ACS patients with plaque erosion and guide them to conservative management without invasive procedures. The results of this exploratory analysis need to be confirmed in large scale prospective clinical studies. Clinical Trial Registration URL: http://www.clinicaltrials.gov. Unique identifier: NCT03479723.
Keywords: acute coronary syndrome; optical coherence tomography; plaque erosion.
Figures
References
-
- Jia H, Abtahian F, Aguirre AD, Lee S, Chia S, Lowe H, Kato K, Yonetsu T, Vergallo R, Hu S, Tian J, Lee H, Park S‐J, Jang YS, Raffel OC, Mizuno K, Uemura S, Itoh T, Kakuta T, Choi S‐Y, Dauerman HL, Prasad A, Toma C, McNulty I, Zhang S, Yu B, Fuster V, Narula J, Virmani R, Jang I‐K. In vivo diagnosis of plaque erosion and calcified nodule in patients with acute coronary syndrome by intravascular optical coherence tomography. J Am Coll Cardiol. 2013;62:1748–1758. - PMC - PubMed
-
- Higuma T, Soeda T, Abe N, Yamada M, Yokoyama H, Shibutani S, Vergallo R, Minami Y, Ong DS, Lee H, Okumura K, Jang IK. A combined optical coherence tomography and intravascular ultrasound study on plaque rupture, plaque erosion, and calcified nodule in patients with ST‐segment elevation myocardial infarction. JACC Cardiovasc Interv. 2015;8:1166–1176. - PubMed
-
- Falk E, Nakano M, Bentzon JF, Finn AV, Virmani R. Update on acute coronary syndromes: the pathologists’ view. Eur Heart J. 2013;34:719–728. - PubMed
-
- Roffi M, Patrono C, Collet JP, Mueller C, Valgimigli M, Andreotti F, Bax JJ, Borger MA, Brotons C, Chew DP, Gencer B, Hasenfuss G, Kjeldsen K, Lancellotti P, Landmesser U, Mehilli J, Mukherjee D, Storey RF, Windecker S; ESC Scientific Document Group . 2015 ESC guidelines for the management of acute coronary syndromes in patients presenting without persistent ST‐segment elevation: Task Force for the management of acute coronary syndromes in patients presenting without persistent ST‐segment elevation of the European Society of Cardiology (ESC). Eur Heart J. 2016;37:267–315. - PubMed
-
- Amsterdam EA, Wenger NK, Brindis RG, Casey DE, Ganiats TG, Holmes DR, Jaffe AS, Jneid H, Kelly RF, Kontos MC, Levine GN, Liebson PR, Mukherjee D, Peterson ED, Sabatine MS, Smalling RW, Zieman SJ; ACC/AHA Task Force Members . 2014 AHA/ACC guideline for the management of patients with non‐ST‐elevation acute coronary syndromes: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;130:e344–e426. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
