

Effects of exenatide and open-label SGLT2 inhibitor treatment, given in parallel or sequentially, on mortality and cardiovascular and renal outcomes in type 2 diabetes: insights from the EXSCEL trial
- PMID: 31640705
- PMCID: PMC6805385
- DOI: 10.1186/s12933-019-0942-x
Effects of exenatide and open-label SGLT2 inhibitor treatment, given in parallel or sequentially, on mortality and cardiovascular and renal outcomes in type 2 diabetes: insights from the EXSCEL trial
Abstract
Background: Sodium-glucose cotransporter-2 inhibitors (SGLT2i) and glucagon-like peptide-1 receptor agonists (GLP-1 RA) improve cardiovascular and renal outcomes in patients with type 2 diabetes through distinct mechanisms. However, evidence on clinical outcomes in patients treated with both GLP-1 RA and SGLT2i is lacking. We aim to provide insight into the effects of open-label SGLT2i use in parallel with or shortly after once-weekly GLP-1 RA exenatide (EQW) on cardiorenal outcomes.
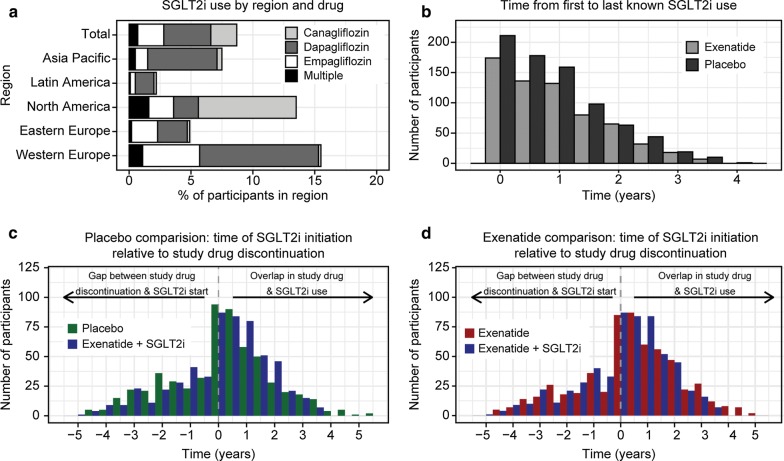
Methods: In the EXSCEL cardiovascular outcomes trial EQW arm, SGLT2i drop-in occurred in 8.7% of participants. These EQW+SGLT2i users were propensity-matched to: (1) placebo-arm participants not taking SGLT2i (n = 572 per group); and to (2) EQW-arm participants not taking SGLT2i (n = 575), based on their last measured characteristics before SGLT2i initiation, and equivalent study visit in comparator groups. Time-to-first major adverse cardiovascular event (MACE) and all-cause mortality (ACM) were compared using Cox regression analyses. eGFR slopes were quantified using mixed model repeated measurement analyses.
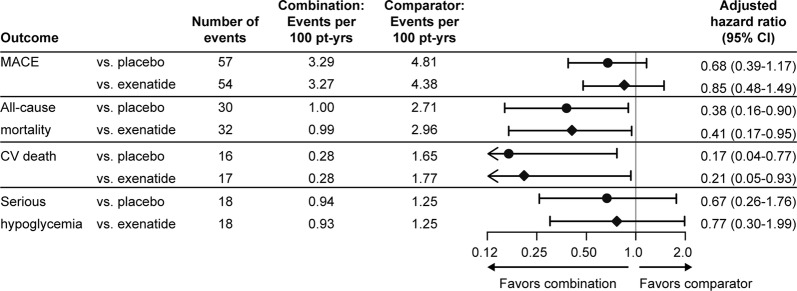
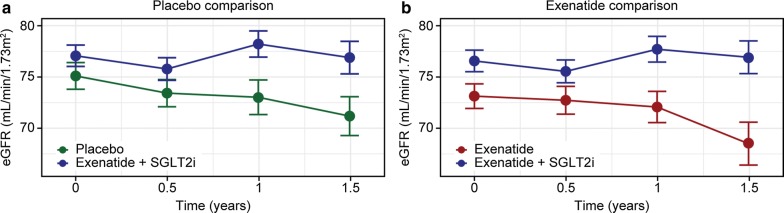
Results: In adjusted analyses, the risk for MACE with combination EQW+SGLT2i use was numerically lower compared with both placebo (adjusted hazard ratio 0.68, 95% CI 0.39-1.17) and EQW alone (0.85, 0.48-1.49). Risk of ACM was nominally significantly reduced compared with placebo (0.38, 0.16-0.90) and compared with EQW (0.41, 0.17-0.95). Combination EQW+SGLT2i use also nominally significantly improved estimated eGFR slope compared with placebo (+ 1.94, 95% CI 0.94-2.94 mL/min/1.73 m2/year) and EQW alone (+ 2.38, 1.40-3.35 mL/min/1.73 m2/year).
Conclusions: This post hoc analysis supports the hypothesis that combinatorial EQW and SGLT2i therapy may provide benefit on cardiovascular outcomes and mortality. Trial registration Clinicaltrials.gov, Identifying number: NCT01144338, Date of registration: June 15, 2010.
Keywords: Cardiovascular outcomes; Combination therapy; Exenatide; GLP-1 receptor agonist; Propensity score matching; SGLT2 inhibitor; Type 2 diabetes mellitus; eGFR slope.
Conflict of interest statement
LEC, RCP, SB, DWB, SG, CDS, and JR are employees and/or shareholders of AstraZeneca. SG’s spouse is also an employee of AstraZeneca. HJLH serves on advisory panels for Boehringer Ingelheim GmbH and Merck & Co., Inc, and is a consultant for AbbVie Inc., AstraZeneca, Fresenius SE & Co. KGaA, Janssen Research & Development, and Mitsubishi Tanabe Pharma Corporation. RCP is a stockholder of Novartis Pharmaceuticals Corporation. DWB is a stockholder of Bristol-Myers Squibb Company. MT is a consultant for AstraZeneca. RJM has received research support and honoraria from AstraZeneca, GlaxoSmithKline plc., and Merck & Co., Inc. AFH is a consultant for Bayer AG & Boehringer Ingelheim Pharmaceuticals, Inc., and receives research support from AstraZeneca, GlaxoSmithKline plc., Janssen Pharmaceuticals, Inc., Merck & Co., Inc., and Novartis Pharmaceuticals Corporation. RRH has attended advisory boards at Elcelyx Therapeutics, Inc., Merck & Co., Inc., Novartis AG, Novo Nordisk A/S, Amylin, and Eli Lilly. RRH has given lectures supported by Bayer AG, Eli Lilly, Merck & Co., Inc, and Novo Nordisk A/S, and received research support and honoraria from AstraZeneca, Bayer AG, and Merck & Co., Inc. RRH is an Emeritus NIHR Senior Investigator. JBB’s contracted consulting fees are paid to the University of North Carolina by Adocia, AstraZeneca, Dance Biopharm, Eli Lilly, MannKind, NovaTarg, Novo Nordisk, Senseonics, vTv Therapeutics, and Zafgen; grant support from Novo Nordisk, Sanofi, and vTv Therapeutics. He is a consultant to Cirius Therapeutics Inc, CSL Behring, Neurimmune AG, and Whole Biome Inc. He holds stock options in Mellitus Health, PhaseBio, Stability Health, and Whole Biome Inc. He is supported by a grant from the National Institutes of Health (UL1TR002489).
Figures
References
-
- Zelniker TA, Wiviott SD, Raz I, Im K, Goodrich EL, Bonaca MP, et al. SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes: a systematic review and meta-analysis of cardiovascular outcome trials. Lancet. 2019 doi: 10.1016/s0140-6736(18)32590-x. - DOI - PubMed
-
- Zelniker Thomas A, Wiviott Stephen D, Raz I, Im K, Goodrich Erica L, Furtado Remo HM, et al. Comparison of the effects of glucagon-like peptide receptor agonists and sodium-glucose co-transporter 2 inhibitors for prevention of major adverse cardiovascular and renal outcomes in type 2 diabetes mellitus: a systematic review and meta-analysis of cardiovascular outcomes trials. Circulation. 2019 doi: 10.1161/circulationaha.118.038868. - DOI - PubMed
-
- Hussein H, Zaccardi F, Khunti K, Seidu S, Davies MJ, Gray LJ. Cardiovascular efficacy and safety of sodium-glucose co-transporter-2 inhibitors and glucagon-like peptide-1 receptor agonists: a systematic review and network meta-analysis. Diabetic Med. 2019;36(4):444–452. doi: 10.1111/dme.13898. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
