

Diabetic cardiomyopathy: Pathophysiology, theories and evidence to date
- PMID: 31641426
- PMCID: PMC6801309
- DOI: 10.4239/wjd.v10.i10.490
Diabetic cardiomyopathy: Pathophysiology, theories and evidence to date
Abstract
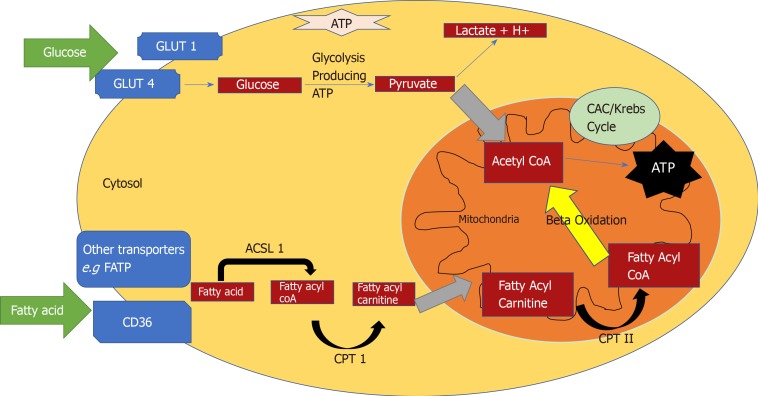
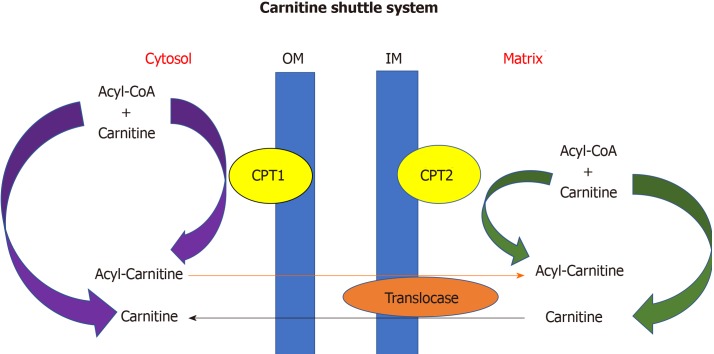
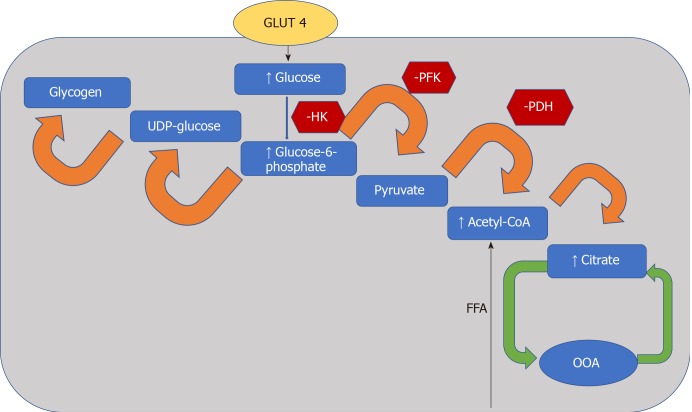
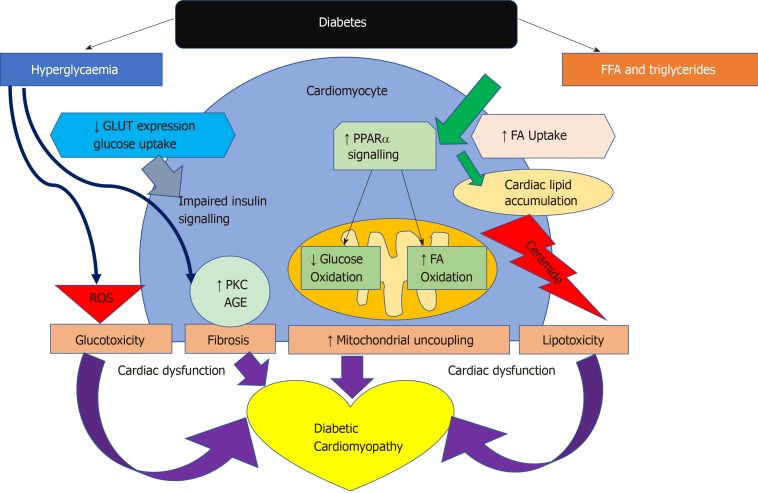
The prevalence of type 2 diabetes (T2D) has increased worldwide and doubled over the last two decades. It features among the top 10 causes of mortality and morbidity in the world. Cardiovascular disease is the leading cause of complications in diabetes and within this, heart failure has been shown to be the leading cause of emergency admissions in the United Kingdom. There are many hypotheses and well-evidenced mechanisms by which diabetic cardiomyopathy as an entity develops. This review aims to give an overview of these mechanisms, with particular emphasis on metabolic inflexibility. T2D is associated with inefficient substrate utilisation, an inability to increase glucose metabolism and dependence on fatty acid oxidation within the diabetic heart resulting in mitochondrial uncoupling, glucotoxicity, lipotoxicity and initially subclinical cardiac dysfunction and finally in overt heart failure. The review also gives a concise update on developments within clinical imaging, specifically cardiac magnetic resonance studies to characterise and phenotype early cardiac dysfunction in T2D. A better understanding of the pathophysiology involved provides a platform for targeted therapy in diabetes to prevent the development of early heart failure with preserved ejection fraction.
Keywords: Cardiac metabolism; Diabetic cardiomyopathy; Myocardial steatosis; Myocardial strain.
©The Author(s) 2019. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: No potential conflicts of interest.
Figures
References
-
- WHO. Diabetes Fact Sheet. World Health Organisation, Geneva. Available from: https://www.who.int/en/news-room/fact-sheets/detail/diabetes.
-
- WHO. The top 10 causes of death [updated May 2018]. World Health Organization, Geneva. Available from: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death.
-
- Kannel WB, McGee DL. Diabetes and cardiovascular disease. The Framingham study. JAMA. 1979;241:2035–2038. - PubMed
-
- NHS Trusts. National Diabetes Audit Complications and Mortality 2015-2016. Available from: https://digital.nhs.uk/data-and-information/publications/statistical/nat....
