

Surgical outcomes in adults with purpura fulminans: a systematic review and patient-level meta-synthesis
- PMID: 31641673
- PMCID: PMC6798408
- DOI: 10.1186/s41038-019-0168-x
Surgical outcomes in adults with purpura fulminans: a systematic review and patient-level meta-synthesis
Abstract
Background: Cutaneous manifestations of purpura fulminans (PF) present many challenges for clinicians and surgeons. In a state of septic shock complicated by limb ischemia, surgical interventions are necessary to control the pathological cascade and improve patient outcomes. The objective of this article was to report etiologies and surgical outcomes associated with cutaneous manifestations in adults.
Methods: This systematic review and meta-analysis compared 190 adult patients with etiologies, signs and symptoms, and surgical outcomes associated with cutaneous manifestations of PF. The PubMed, EMBASE, Cochrane Library, Web of Science, and Scopus databases were systematically and independently searched. Patient and clinical characteristics, surgical interventions, outcomes, and complications were recorded.
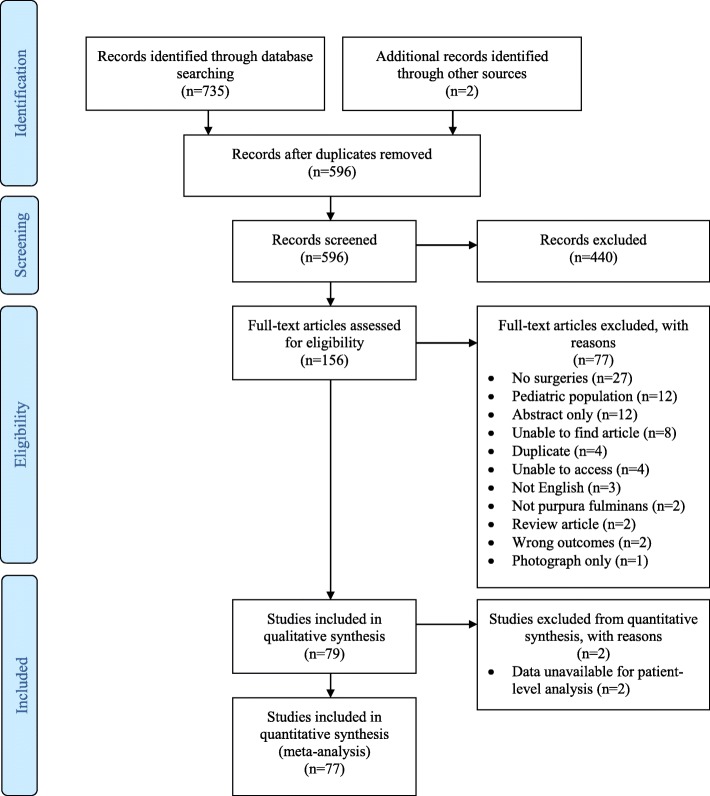
Results: Seventy-nine studies were eligible for the systematic review, and 77 were eligible for meta-analysis using Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) and Cochrane guidelines. A total of 71/190 (38%) cases reported surgical debridement. Fasciotomies were reported in 12/190 (6%) cases and 20 procedures. Amputations were reported in 154/190 (81%) cases. Reconstruction was reported in 45 cases. Skin grafts were applied in 31 cases. Flaps were used for reconstruction in 28 cases. Median (IQR) surgical procedures per patient were 4 (4, 5) procedures. Infectious organisms causing PF were 32% Neisseria meningitidis (n = 55) and 32% Streptococcus pneumonia (n = 55). Coagulase-negative Staphylococcus (95% confidence interval (CI)(8.2-177.9), p = 0.032), Haemophilus influenza (95%CI (7.2-133), p = 0.029), Streptococcus pneumonia (95% CI (13.3-75.9), p = 0.006), and West Nile Virus (95%CI (8.2-177.9), p = 0.032) were associated with significantly more extensive amputations compared to other organisms.
Conclusion: This systematic review and patient-level meta-analysis found the most common presentation of PF was septic shock from an infectious organism. Neisseria meningitidis and Streptococcus pneumonia were equally the most common organisms associated with PF. The majority of cases were not treated in a burn center. The most common surgeries were amputations, with below-the-knee-amputations being the most common procedure. Skin grafting was the most commonly performed reconstructive procedure. The most common complications were secondary infections. Organisms with significantly more extensive amputations were coagulase-negative Staphylococcus, Haemophilus influenza, Streptococcus pneumonia, and West Nile Virus. Interpretation of findings should be cautioned due to limited sample data.
Keywords: Amputation; Burn units; Neisseria; Purpura fulminans; Reconstructive surgical procedures; Septic; Shock; Surgeons; Treatment outcome.
© The Author(s) 2019.
Conflict of interest statement
Competing interestsThe authors declare that they have no competing interests.
Figures

References
-
- Guelliot A. Note sur trois cas de purpura infectieux foudroyant. Union med et scient du nord-est. 1884;8:25–37.
Publication types
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
