

Antibiotic Prescribing Variability in a Large Urgent Care Network: A New Target for Outpatient Stewardship
- PMID: 31641768
- PMCID: PMC7768670
- DOI: 10.1093/cid/ciz910
Antibiotic Prescribing Variability in a Large Urgent Care Network: A New Target for Outpatient Stewardship
Abstract
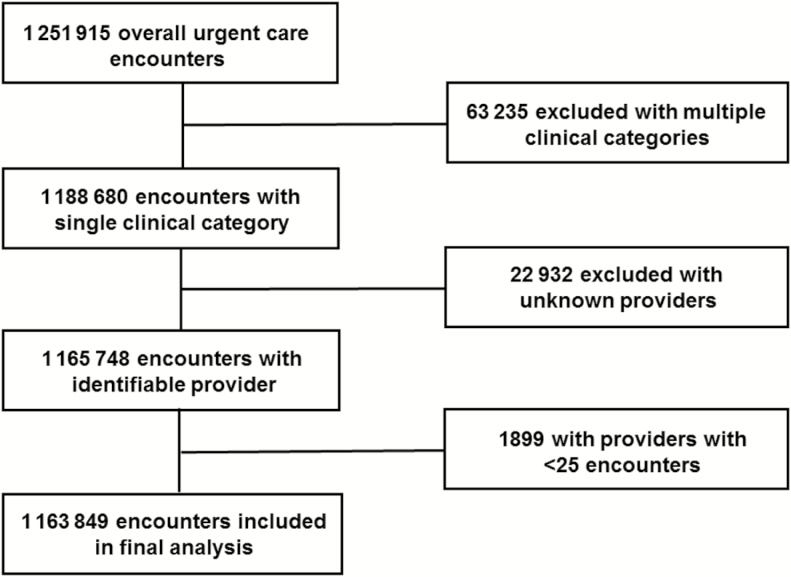
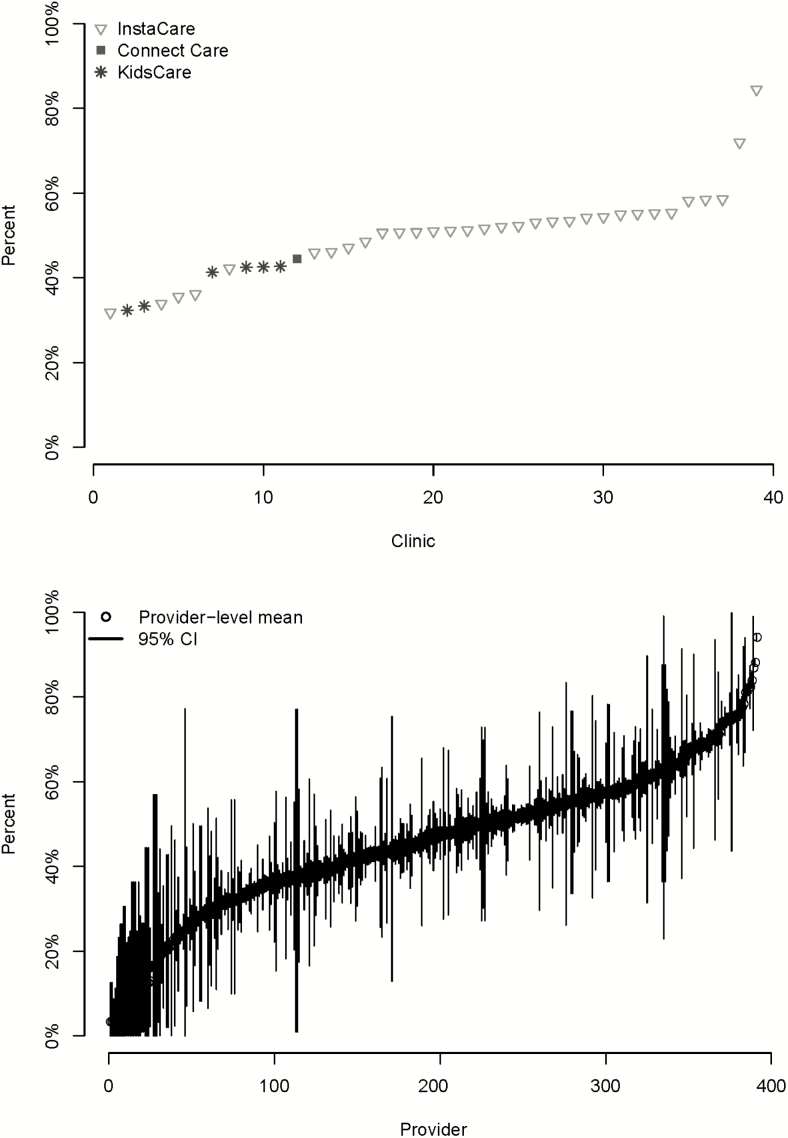
Improving antibiotic prescribing in outpatient settings is a public health priority. In the United States, urgent care (UC) encounters are increasing and have high rates of inappropriate antibiotic prescribing. Our objective was to characterize antibiotic prescribing practices during UC encounters, with a focus on respiratory tract conditions. This was a retrospective cohort study of UC encounters in the Intermountain Healthcare network. Among 1.16 million UC encounters, antibiotics were prescribed during 34% of UC encounters and respiratory conditions accounted for 61% of all antibiotics prescribed. Of respiratory encounters, 50% resulted in antibiotic prescriptions, yet the variability at the level of the provider ranged from 3% to 94%. Similar variability between providers was observed for respiratory conditions where antibiotics were not indicated and in first-line antibiotic selection for sinusitis, otitis media, and pharyngitis. These findings support the importance of developing antibiotic stewardship interventions specifically targeting UC settings.
Keywords: antibiotic stewardship; pediatric urgent care; telemedicine; urgent care.
Published by Oxford University Press for the Infectious Diseases Society of America 2019. This work is written by (a) US Government employee(s) and is in the public domain in the US.
Figures
References
-
- Frost HM, Knepper BC, Shihadeh KC, Jenkins TC. A novel approach to evaluate antibiotic utilization across the spectrum of inpatient and ambulatory care and implications for prioritization of antibiotic stewardship efforts. Clin Infect Dis 2019. PMID: 31162539. - PubMed
-
- Fleming-Dutra KE, Hersh AL, Shapiro DJ, et al. . Prevalence of inappropriate antibiotic prescriptions among US ambulatory care visits, 2010-2011. JAMA 2016; 315:1864–73. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
