

Prediction of Sex-Specific Suicide Risk Using Machine Learning and Single-Payer Health Care Registry Data From Denmark
- PMID: 31642880
- PMCID: PMC6813578
- DOI: 10.1001/jamapsychiatry.2019.2905
Prediction of Sex-Specific Suicide Risk Using Machine Learning and Single-Payer Health Care Registry Data From Denmark
Erratum in
-
Errors in Abstract, Statistical Analysis, and Results.JAMA Psychiatry. 2020 Jan 1;77(1):103-104. doi: 10.1001/jamapsychiatry.2019.4110. JAMA Psychiatry. 2020. PMID: 31799988 Free PMC article. No abstract available.
Abstract
Importance: Suicide is a public health problem, with multiple causes that are poorly understood. The increased focus on combining health care data with machine-learning approaches in psychiatry may help advance the understanding of suicide risk.
Objective: To examine sex-specific risk profiles for death from suicide using machine-learning methods and data from the population of Denmark.
Design, setting, and participants: A case-cohort study nested within 8 national Danish health and social registries was conducted from January 1, 1995, through December 31, 2015. The source population was all persons born or residing in Denmark as of January 1, 1995. Data were analyzed from November 5, 2018, through May 13, 2019.
Exposures: Exposures included 1339 variables spanning domains of suicide risk factors.
Main outcomes and measures: Death from suicide from the Danish cause of death registry.
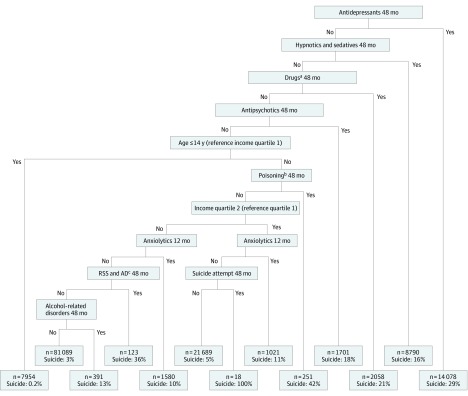
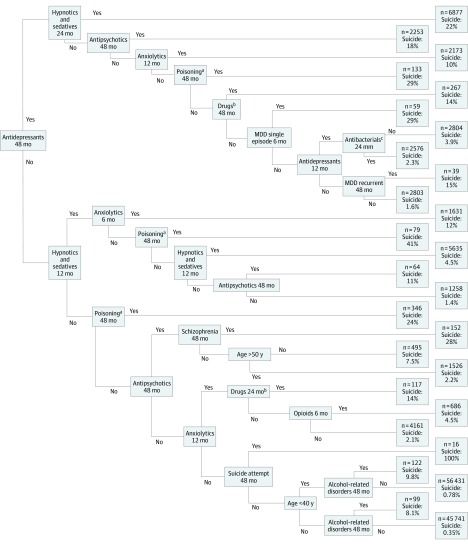
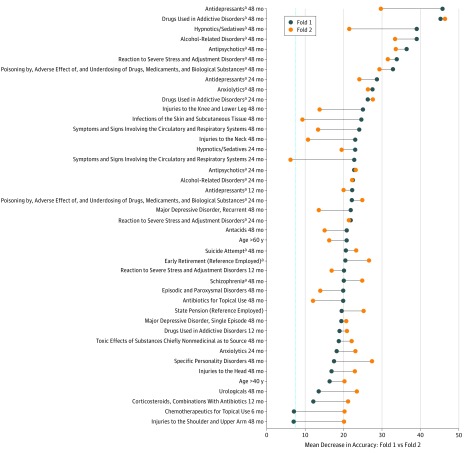
Results: A total of 14 103 individuals died by suicide between 1995 and 2015 (10 152 men [72.0%]; mean [SD] age, 43.5 [18.8] years and 3951 women [28.0%]; age, 47.6 [18.8] years). The comparison subcohort was a 5% random sample (n = 265 183) of living individuals in Denmark on January 1, 1995 (130 591 men [49.2%]; age, 37.4 [21.8] years and 134 592 women [50.8%]; age, 39.9 [23.4] years). With use of classification trees and random forests, sex-specific differences were noted in risk for suicide, with physical health more important to men's suicide risk than women's suicide risk. Psychiatric disorders and possibly associated medications were important to suicide risk, with specific results that may increase clarity in the literature. Generally, diagnoses and medications measured 48 months before suicide were more important indicators of suicide risk than when measured 6 months earlier. Individuals in the top 5% of predicted suicide risk appeared to account for 32.0% of all suicide cases in men and 53.4% of all cases in women.
Conclusions and relevance: Despite decades of research on suicide risk factors, understanding of suicide remains poor. In this study, the first to date to develop risk profiles for suicide based on data from a full population, apparent consistency with what is known about suicide risk was noted, as well as potentially important, understudied risk factors with evidence of unique suicide risk profiles among specific subpopulations.
Conflict of interest statement
Figures

Comment in
-
Machine Learning for Suicide Research-Can It Improve Risk Factor Identification?JAMA Psychiatry. 2020 Jan 1;77(1):13-14. doi: 10.1001/jamapsychiatry.2019.2896. JAMA Psychiatry. 2020. PMID: 31642876 Free PMC article. No abstract available.
References
-
- World Health Organization Suicide rate estimates, age-standardized estimates by country. http://apps.who.int/gho/data/node.main.MHSUICIDEASDR?lang=en. Updated July 17, 2018. Accessed January 18, 2019.
-
- Suicide Prevention Resource Center. Research Prioritization Task Force, National Action Alliance for Suicide Prevention A prioritized research agenda for suicide prevention: an action plan to save lives. https://www.sprc.org/resources-programs/prioritized-research-agenda-suic.... Published 2014. Accessed January 18, 2019.
-
- Murphy S, Xu J, Kochanek K, Arias E Mortality in the United States, 2017. Report No.: NCHS Data Brief, no 328. https://www.cdc.gov/nchs/products/databriefs/db328.htm. Published November 2018. Accessed January 18, 2019 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
