

The natural history of seizures and neuropsychiatric symptoms in childhood epilepsy with centrotemporal spikes (CECTS)
- PMID: 31645314
- PMCID: PMC8087164
- DOI: 10.1016/j.yebeh.2019.07.038
The natural history of seizures and neuropsychiatric symptoms in childhood epilepsy with centrotemporal spikes (CECTS)
Abstract
Objective: Childhood epilepsy with centrotemporal spikes (CECTS) (formally benign epilepsy with centrotemporal spikes, BECTS) is a common childhood epilepsy syndrome characterized by psychiatric, behavioral, and cognitive abnormalities and self-limited seizures. Although CECTS is one of the most well-characterized electroclinical epilepsy syndromes, the natural history of neuropsychiatric outcomes is poorly understood. We report the psychiatric, behavioral, and cognitive profiles over the course of disease from a large, prospectively-enrolled, longitudinal cohort of children with CECTS. We further characterize the detailed seizure course and test the relationship between several proposed risk factors and neuropsychiatric and seizure outcomes in these children.
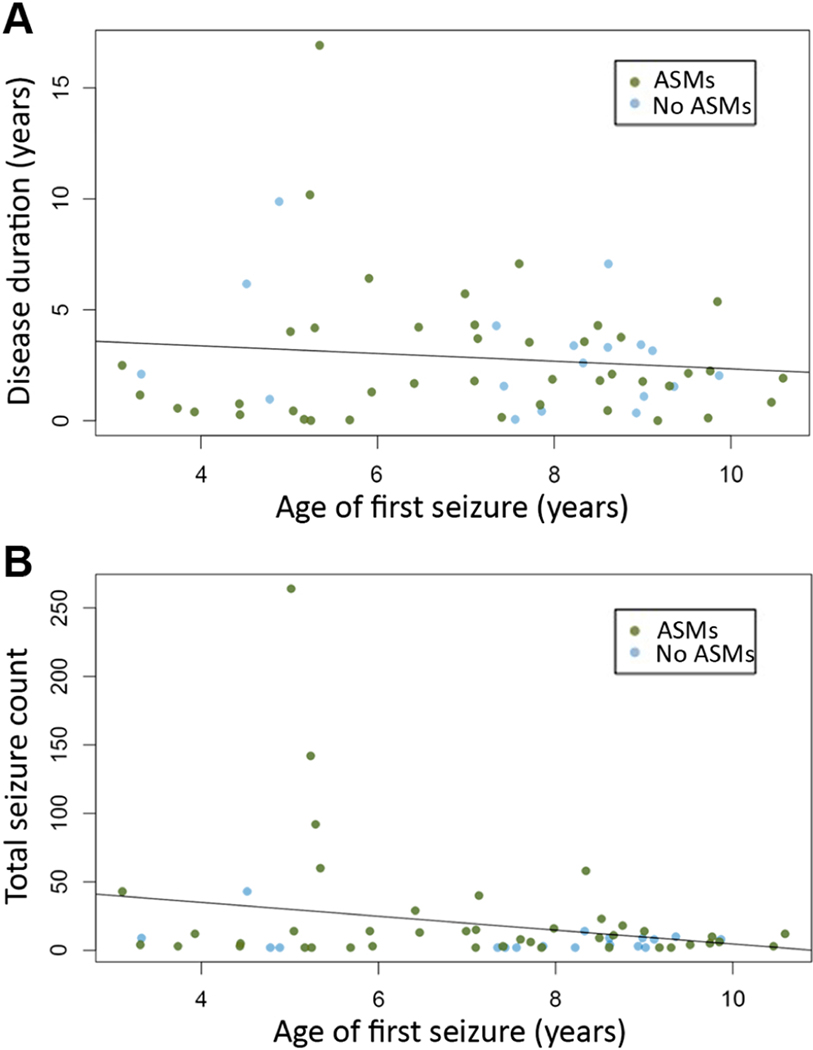
Methods: Patients diagnosed with CECTS were enrolled as part of a community-based study and followed from diagnosis through disease resolution (16.0 ± 3.1 years, N = 60). Twenty sibling controls were also recruited. We report the natural history of premorbid neuropsychiatric concerns, postmorbid neuropsychiatric diagnoses, long-term neuropsychological performance, seizure course, antiseizure medication (ASM) treatment response, and the relationship between duration seizure-free and remission. Age at onset and premorbid neuropsychiatric concerns were tested as predictors of seizure count, epilepsy duration, postmorbid neuropsychiatric diagnoses, and long-term neuropsychological performance. Antiseizure medication treatment duration, seizure count, and epilepsy duration were tested as predictors of postmorbid neuropsychiatric diagnoses and long-term neuropsychological performance.
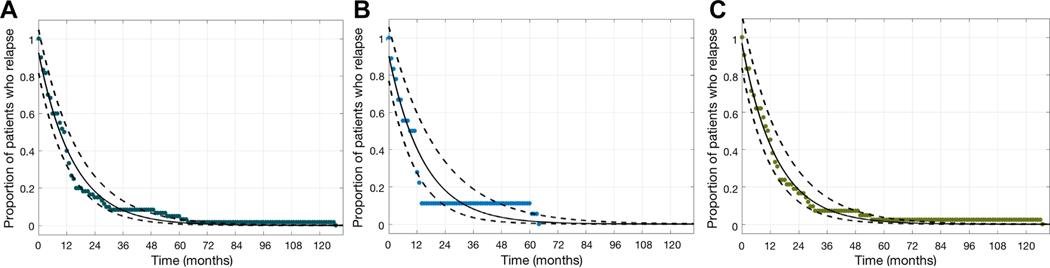
Results: Children with CECTS had a high incidence of ADD/ADHD symptoms (18.3%) or learning difficulties (21.7%) before diagnosis. New or persistent ADHD (20%), mood disorders (23.6%), learning difficulties (14.5%), and behavioral disorders (7.3%) were common after CECTS diagnosis. At 9-year follow-up, performance on formal neuropsychological testing was comparable to population statistics and sibling controls. More than two-thirds of treated children experienced at least one seizure during treatment. Most children (61.7%) had entered terminal resolution after 12 months seizure-free. Among all children, for each month seizure-free, there was a 6-7% increase in the probability of achieving terminal remission (p < 1e-10). The presence of a premorbid neurodevelopmental concern predicted a longer epilepsy duration (p = 0.02), higher seizure count (p = 0.02), and a postmorbid psychiatric or neurodevelopmental diagnosis (p = 0.002). None of the tested features predicted long-term neuropsychological performance.
Significance: Children are at high risk of neuropsychiatric symptoms along the course of the disease in CECTS, however, long-term cognitive performance is favorable. The majority of children had a seizure while being treated with ASMs, suggesting that CECTS is not as pharmacoresponsive as assumed or that treatment approaches are not optimized. Among treated and untreated children, future seizure-risk can be estimated from duration seizure-free. The presence of a premorbid neuropsychiatric concern predicted a more severe disease course in CECTS.
Keywords: Behavior; Cognitive; Mood; Outcome; Rolandic; Treatment.
Copyright © 2019 Elsevier Inc. All rights reserved.
Figures


References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
