

A six-gene leukemic stem cell score identifies high risk pediatric acute myeloid leukemia
- PMID: 31645648
- PMCID: PMC7135934
- DOI: 10.1038/s41375-019-0604-8
A six-gene leukemic stem cell score identifies high risk pediatric acute myeloid leukemia
Erratum in
-
Correction: A six-gene leukemic stem cell score identifies high risk pediatric acute myeloid leukemia.Leukemia. 2020 Oct;34(10):2821. doi: 10.1038/s41375-020-0822-0. Leukemia. 2020. PMID: 32300185
Abstract
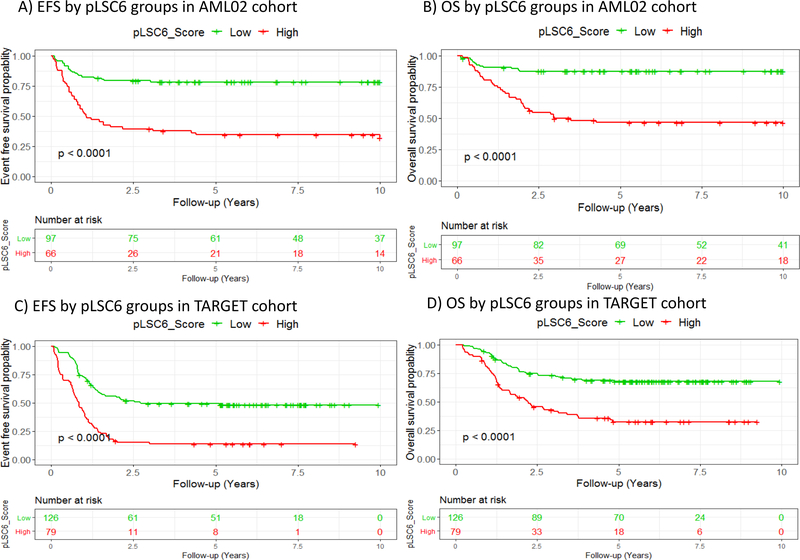
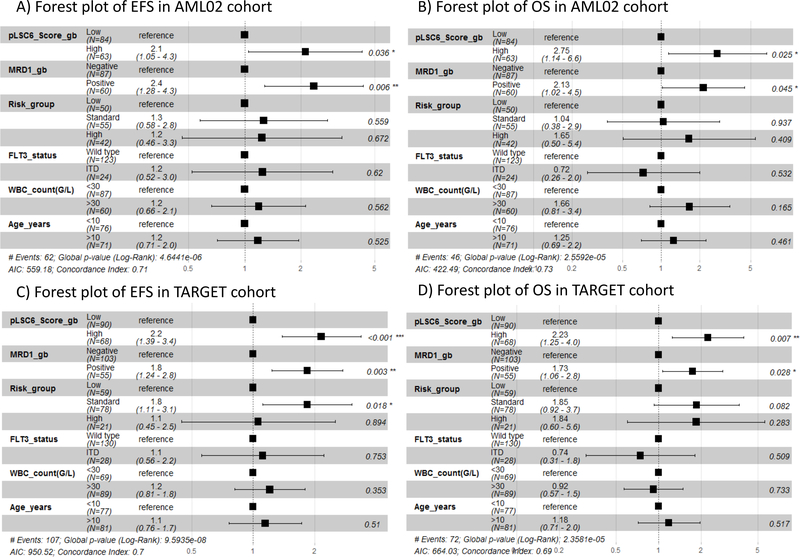
Recently, mRNA-expression signature enriched in LSCs was used to create a 17-gene leukemic stem cell (LSC17) score predictive of prognosis in adult AML. By fitting a Cox-LASSO regression model to the clinical outcome and gene-expression levels of LSC enriched genes in 163 pediatric participants of the AML02 multi-center clinical trial (NCT00136084), we developed a six-gene LSC score of prognostic value in pediatric AML (pLSC6). In the AML02 cohort, the 5-year event-free survival (EFS) of patients within low-pLSC6 group (n = 97) was 78.3 (95% CI = 70.5-86.9%) as compared with 34.5(95% CI = 24.7-48.2 %) in patients within high-pLSC6 group (n = 66 subjects), p < 0.00001. pLSC6 remained significantly associated with EFS and overall survival (OS) after adjusting for induction 1-MRD status, risk-group, FLT3-status, WBC-count at diagnosis and age. pLSC6 formula developed in the AML02 cohort was validated in the pediatric AML-TARGET project data (n = 205), confirming its prognostic value in both single-predictor and multiple-predictor Cox regression models. In both cohorts, pLSC6 predicted outcome of transplant patients, suggesting it as a useful criterion for transplant referrals. Our results suggest that pLSC6 score holds promise in redefining initial risk-stratification and identifying poor risk AML thereby providing guidance for developing novel treatment strategies.
Conflict of interest statement
Figures




References
-
- van Rhenen A, Feller N, Kelder A, Westra AH, Rombouts E, Zweegman S, et al. High stem cell frequency in acute myeloid leukemia at diagnosis predicts high minimal residual disease and poor survival. Clin Cancer Res. 2005;11(18):6520–7. - PubMed
-
- Ng SW, Mitchell A, Kennedy JA, Chen WC, McLeod J, Ibrahimova N, et al. A 17-gene stemness score for rapid determination of risk in acute leukaemia. Nature. 2016;540(7633):433–7. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
