

Fast-track multidisciplinary treatment versus conventional treatment for colorectal cancer: a multicenter, open-label randomized controlled study
- PMID: 31647032
- PMCID: PMC6806550
- DOI: 10.1186/s12885-019-6188-x
Fast-track multidisciplinary treatment versus conventional treatment for colorectal cancer: a multicenter, open-label randomized controlled study
Abstract
Background: Laparoscopic surgery, fast-track perioperative treatment and XELOX chemotherapy are effective strategies for shortening the duration of hospital stay for cancer patients. This trial aimed to clarify the safety and efficacy of the fast-track multidisciplinary treatment (FTMDT) model compared to conventional surgery combined with chemotherapy in Chinese colorectal cancer patients.
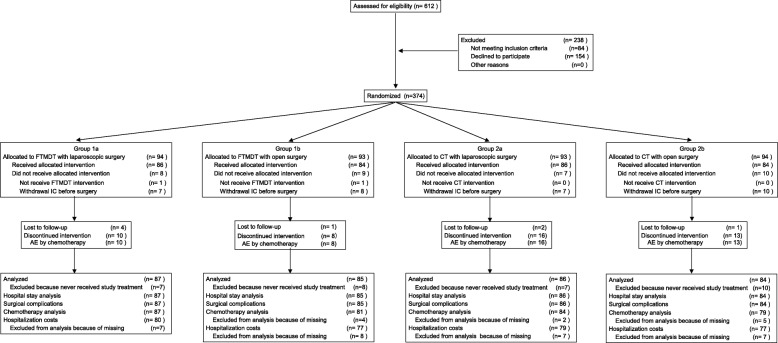
Methods: This trial was a prospective randomized controlled study with a 2 × 2 balanced factorial design and was conducted at six hospitals. Patients in group 1 (FTMDT) received fast-track perioperative treatment and XELOX adjuvant chemotherapy. Patients in group 2 (conventional treatment) received conventional perioperative treatment and mFOLFOX6 adjuvant chemotherapy. Subgroups 1a and 2a had laparoscopic surgery and subgroups 1b and 2b had open surgery. The primary endpoint was total length of hospital stay during treatment.
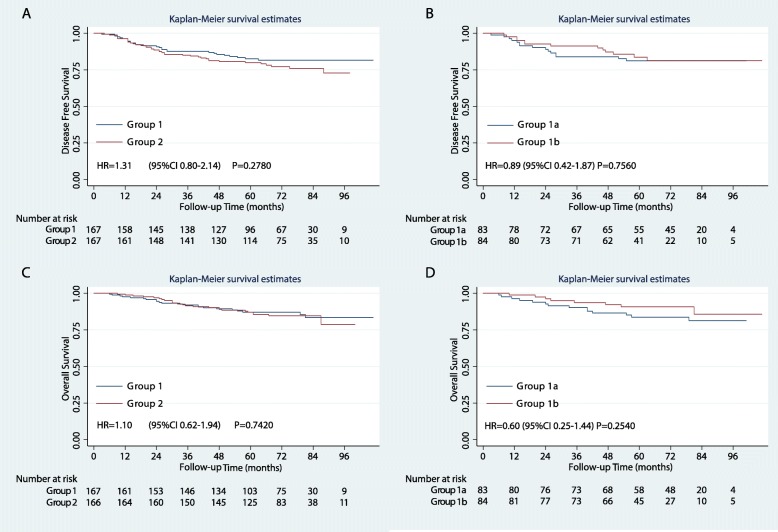
Results: A total of 374 patients were randomly assigned to the four subgroups, and 342 patients were finally analyzed, including 87 patients in subgroup 1a, 85 in subgroup 1b, 86 in subgroup 2a, and 84 in subgroup 2b. The total hospital stay of group 1 was shorter than that of group 2 [13 days, (IQR, 11-17 days) vs. 23.5 days (IQR, 15-42 days), P = 0.0001]. Compared to group 2, group 1 had lower surgical costs, fewer in-hospital complications and faster recovery (all P < 0.05). Subgroup 1a showed faster surgical recovery than that of subgroup 1b (all P < 0.05). There was no difference in 5-year overall survival between groups 1 and 2 [87.1% (95% CI, 80.7-91.5%) vs. 87.1% (95% CI, 80.8-91.4%), P = 0.7420].
Conclusions: The FTMDT model, which integrates laparoscopic surgery, fast-track treatment, and XELOX chemotherapy, was the superior model for enhancing the recovery of Chinese patients with colorectal cancer.
Trial registration: ClinicalTrials.gov: NCT01080547 , registered on March 4, 2010.
Keywords: Colorectal cancer; Colorectal surgery; Randomized controlled trial; Rehabilitation.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Gustafsson UO, Scott MJ, Schwenk W, Demartines N, Roulin D, Francis N, McNaught CE, Macfie J, Liberman AS, Soop M, et al. Guidelines for perioperative care in elective colonic surgery: enhanced recovery after surgery (ERAS((R))) society recommendations. World J Surg. 2013;37(2):259–284. doi: 10.1007/s00268-012-1772-0. - DOI - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
