

Agreement study on gait assessment using a video-assisted rating method in patients with idiopathic normal-pressure hydrocephalus
- PMID: 31648232
- PMCID: PMC6812866
- DOI: 10.1371/journal.pone.0224202
Agreement study on gait assessment using a video-assisted rating method in patients with idiopathic normal-pressure hydrocephalus
Abstract
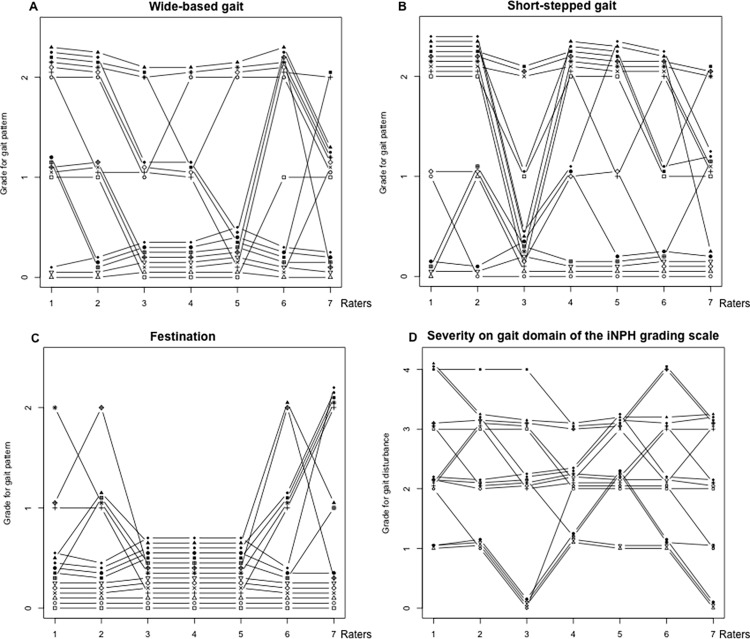
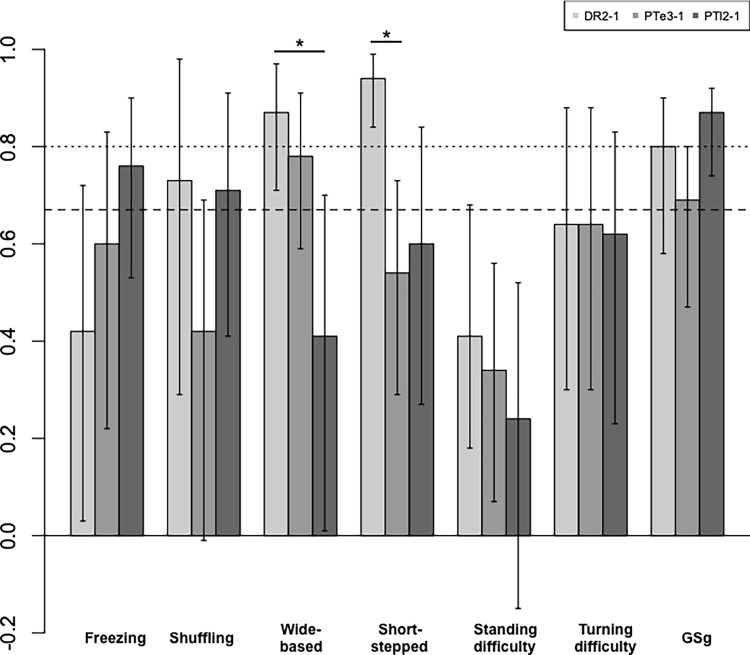
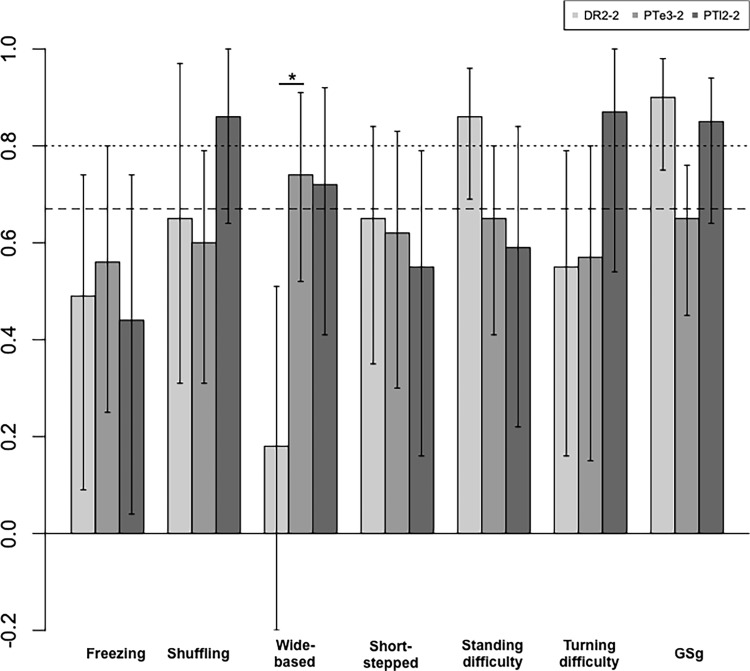
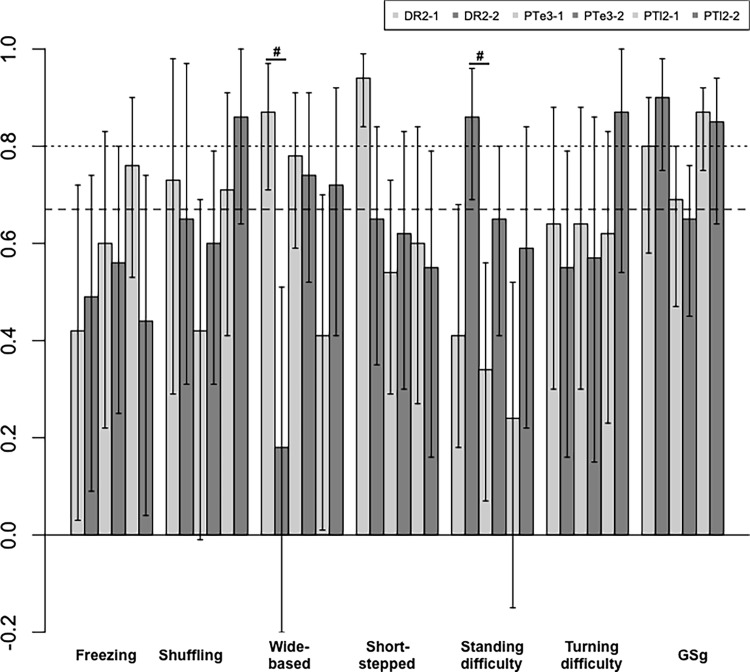
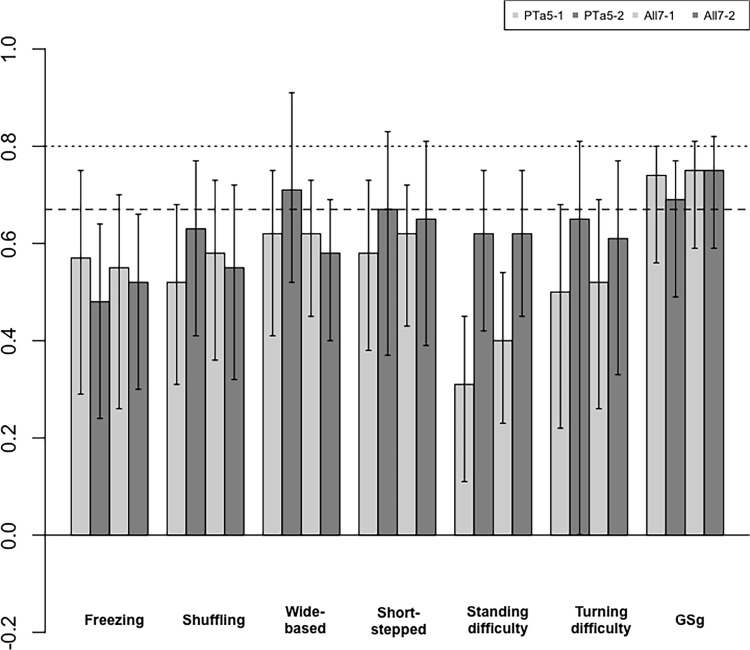
Gait disturbance is a major symptom of idiopathic normal-pressure hydrocephalus (iNPH) and is assessed by raters of different professions or with different degrees of experience. Agreement studies are usually done by two raters or more, and comparisons among multiple groups of raters are rare. In this study, we aimed to examine the agreement among multiple groups of raters on gait patterns and a grading scale through a video-assisted gait analysis in patients with iNPH. Fifteen participants with iNPH were enrolled. Gait was assessed according to seven patterns, including freezing and wide-based gaits. The levels of severity (evident, mild, none) were rated by three groups of raters (two neurosurgeons [DR2], three experienced physiotherapists [PTe3], and two less experienced physiotherapists [PTl2]) through a simultaneous video viewing session. Severity of gait disturbance (GSg) was rated using the Japanese iNPH grading scaleiNPHGS, and Krippendorff alpha was computed to assess agreement, with alpha ≥0.667 indicating good agreement and alpha ≥0.8 indicating excellent agreement. For group comparisons, 84%, not 95%, confidence intervals were applied. Among the seven gait patterns in the first assessment, excellent agreement was observed in wide-based and short-stepped gaits in only DR2. Good agreement was observed in four patterns, but the agreement by two groups was in shuffling and wide-based gait. There were no gait patterns showing good agreement among three groups. In the second assessment, excellent agreement was observed in three patterns but no gait patterns showed good agreement between two groups or more. Learning effect was observed only for standing difficulty in DR2. In contrast, good or nearly good agreement on GSg was observed among the three groups with excellent agreement in two groups. Agreement on gait patterns among the three groups of raters was not high, but agreement on the iNPHGS was high, indicating the importance of a precise description facilitating differentiation between neighboring grades.
Conflict of interest statement
I have read the journal's policy and the authors of this manuscript have the following competing interests: SY received speaker’s honoraria from Johnson & Johnson and Fujifilm Medical Systems. This does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
References
-
- Mori E, Ishikawa M, Kato T, Kazui H, Miyake H, Miyajima M, et al. Guidelines for management of idiopathic normal pressure hydrocephalus: second edition. Neuorol Med Chir. 2012;52:775–809. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
