

Pediatric ALL relapses after allo-SCT show high individuality, clonal dynamics, selective pressure, and druggable targets
- PMID: 31648313
- PMCID: PMC6849953
- DOI: 10.1182/bloodadvances.2019000051
Pediatric ALL relapses after allo-SCT show high individuality, clonal dynamics, selective pressure, and druggable targets
Abstract
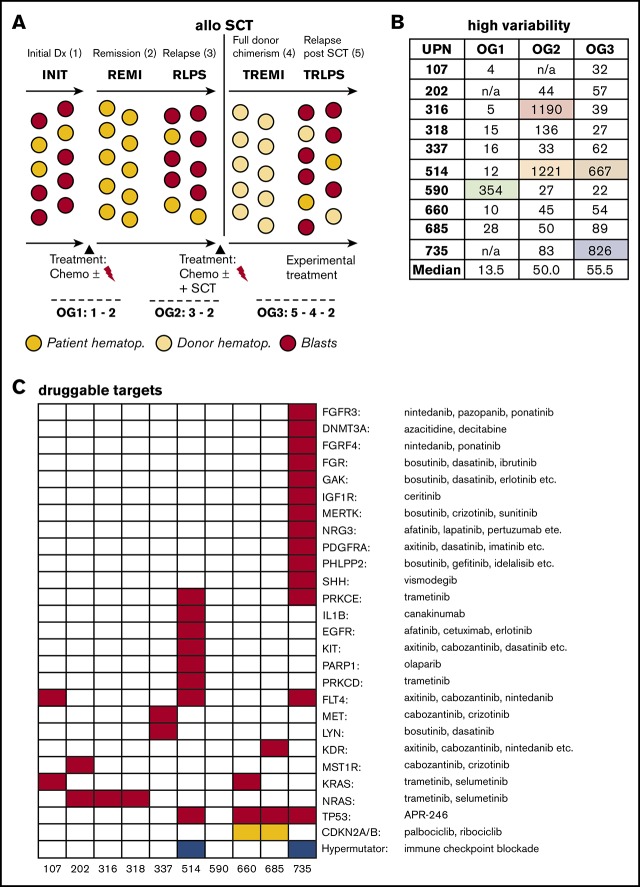
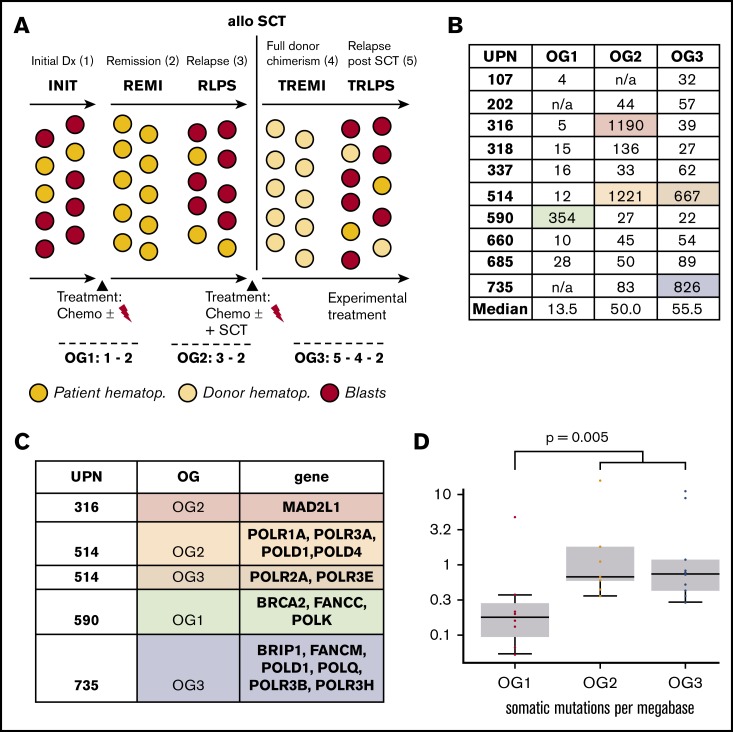
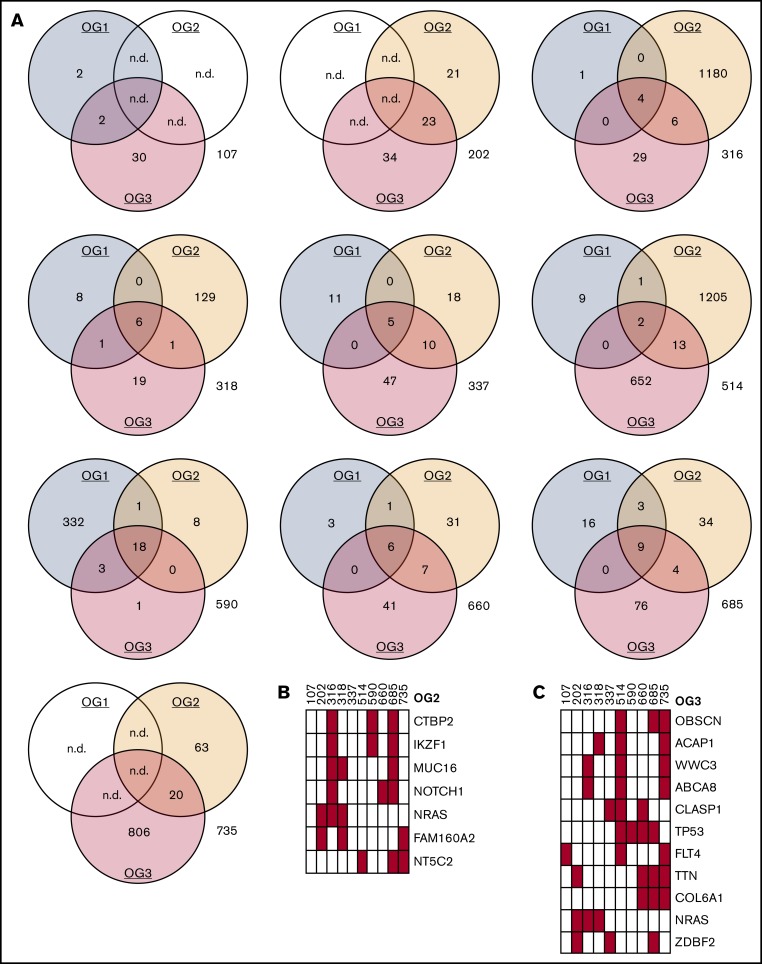
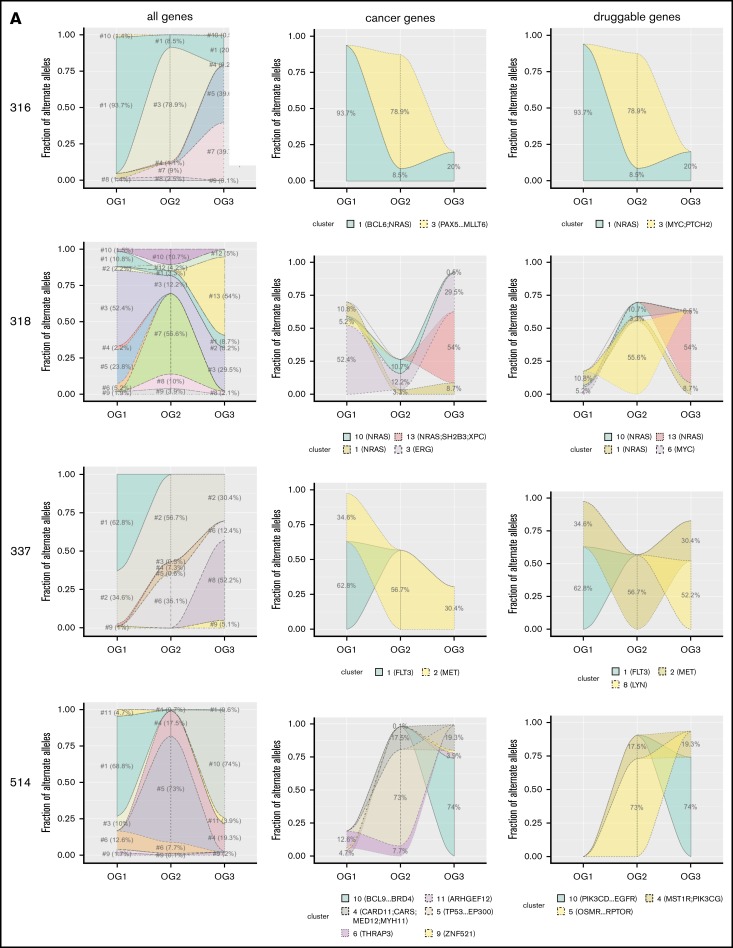
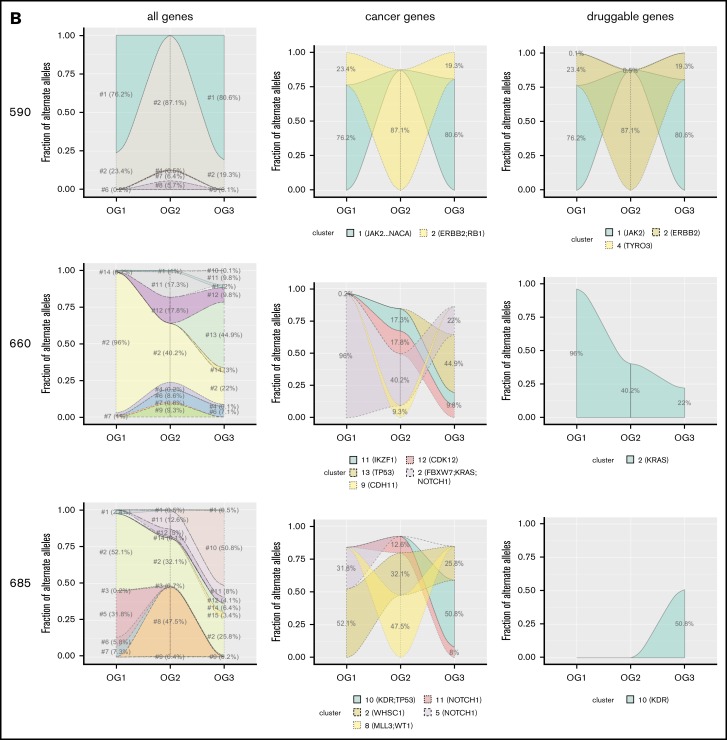
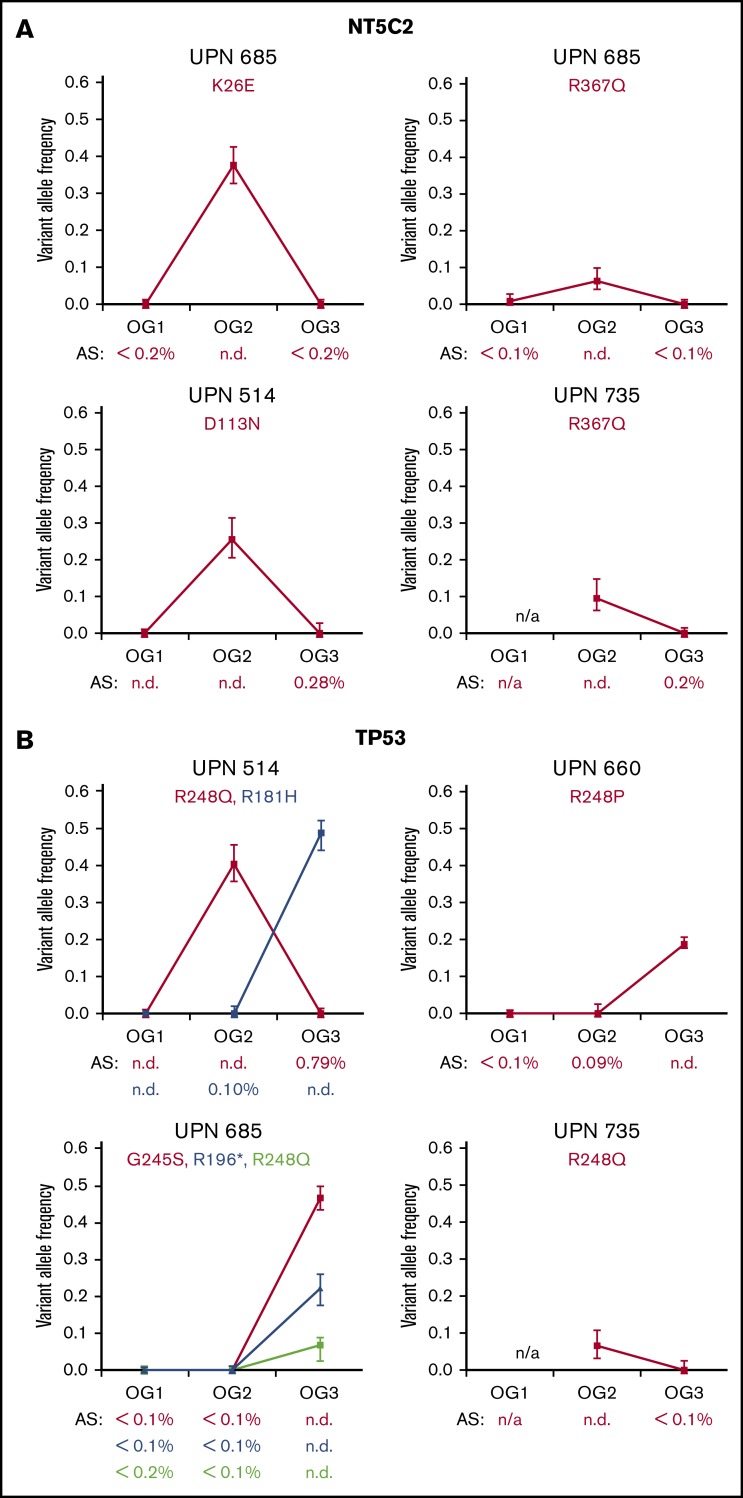
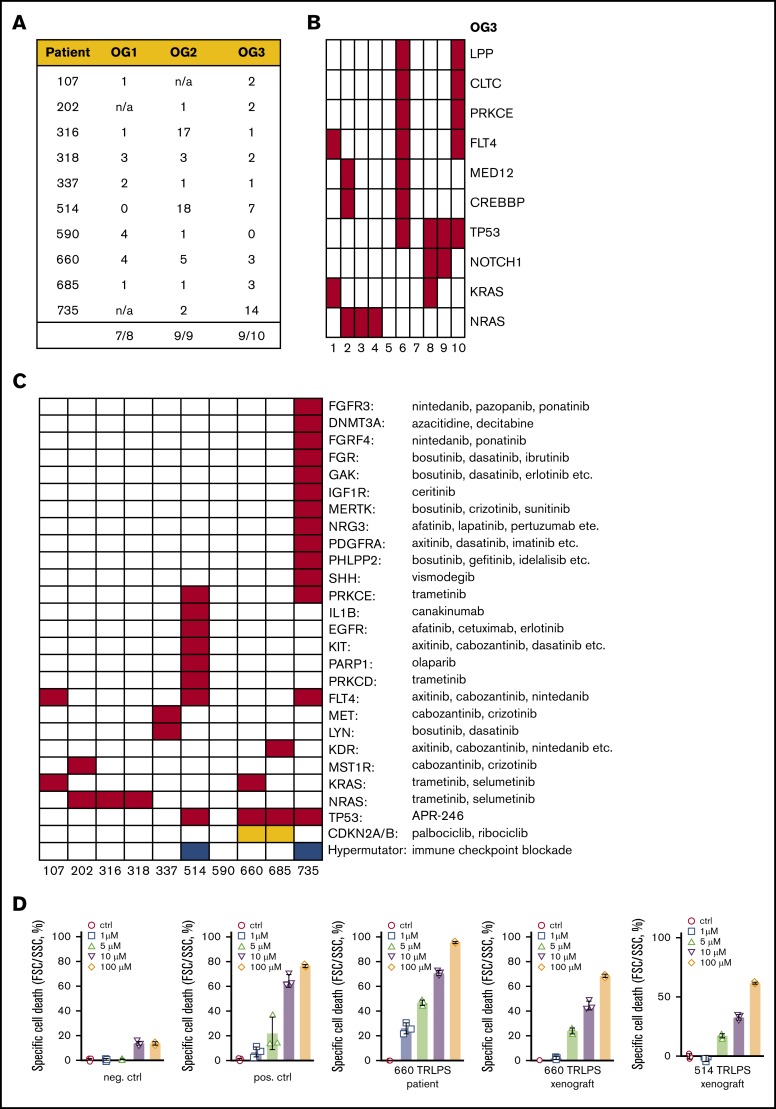
Survival of patients with pediatric acute lymphoblastic leukemia (ALL) after allogeneic hematopoietic stem cell transplantation (allo-SCT) is mainly compromised by leukemia relapse, carrying dismal prognosis. As novel individualized therapeutic approaches are urgently needed, we performed whole-exome sequencing of leukemic blasts of 10 children with post-allo-SCT relapses with the aim of thoroughly characterizing the mutational landscape and identifying druggable mutations. We found that post-allo-SCT ALL relapses display highly diverse and mostly patient-individual genetic lesions. Moreover, mutational cluster analysis showed substantial clonal dynamics during leukemia progression from initial diagnosis to relapse after allo-SCT. Only very few alterations stayed constant over time. This dynamic clonality was exemplified by the detection of thiopurine resistance-mediating mutations in the nucleotidase NT5C2 in 3 patients' first relapses, which disappeared in the post-allo-SCT relapses on relief of selective pressure of maintenance chemotherapy. Moreover, we identified TP53 mutations in 4 of 10 patients after allo-SCT, reflecting acquired chemoresistance associated with selective pressure of prior antineoplastic treatment. Finally, in 9 of 10 children's post-allo-SCT relapse, we found alterations in genes for which targeted therapies with novel agents are readily available. We could show efficient targeting of leukemic blasts by APR-246 in 2 patients carrying TP53 mutations. Our findings shed light on the genetic basis of post-allo-SCT relapse and may pave the way for unraveling novel therapeutic strategies in this challenging situation.
© 2019 by The American Society of Hematology.
Conflict of interest statement
Conflict-of-interest disclosure: P.B. received research support, provided consultancy, and received honoraria (Novartis, Servier, Neovii Biotech, Riemser, Medac). C.P. provided consultancy and speakers bureau service (Medac, Novartis, Jazz Pharma, Amgen, Pfizer). M. Schrappe received research support and honoraria (Novartis, SigmaTau Rare Diseases, JAZZpharma, Amgen). The remaining authors declare no competing financial interests.
Figures
References
-
- Eckert C, Henze G, Seeger K, et al. Use of allogeneic hematopoietic stem-cell transplantation based on minimal residual disease response improves outcomes for children with relapsed acute lymphoblastic leukemia in the intermediate-risk group. J Clin Oncol. 2013;31(21):2736-2742. - PubMed
-
- Tallen G, Ratei R, Mann G, et al. Long-term outcome in children with relapsed acute lymphoblastic leukemia after time-point and site-of-relapse stratification and intensified short-course multidrug chemotherapy: results of trial ALL-REZ BFM 90. J Clin Oncol. 2010;28(14):2339-2347. - PubMed
-
- Peters C, Schrappe M, von Stackelberg A, et al. Stem-cell transplantation in children with acute lymphoblastic leukemia: A prospective international multicenter trial comparing sibling donors with matched unrelated donors-The ALL-SCT-BFM-2003 trial. J Clin Oncol. 2015;33(11):1265-1274. - PubMed
-
- Kato M, Horikoshi Y, Okamoto Y, et al. Second allogeneic hematopoietic SCT for relapsed ALL in children. Bone Marrow Transplant. 2012;47(10):1307-1311. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
