

Corticospinal Tract Injury Estimated From Acute Stroke Imaging Predicts Upper Extremity Motor Recovery After Stroke
- PMID: 31648631
- PMCID: PMC6878199
- DOI: 10.1161/STROKEAHA.119.025898
Corticospinal Tract Injury Estimated From Acute Stroke Imaging Predicts Upper Extremity Motor Recovery After Stroke
Abstract
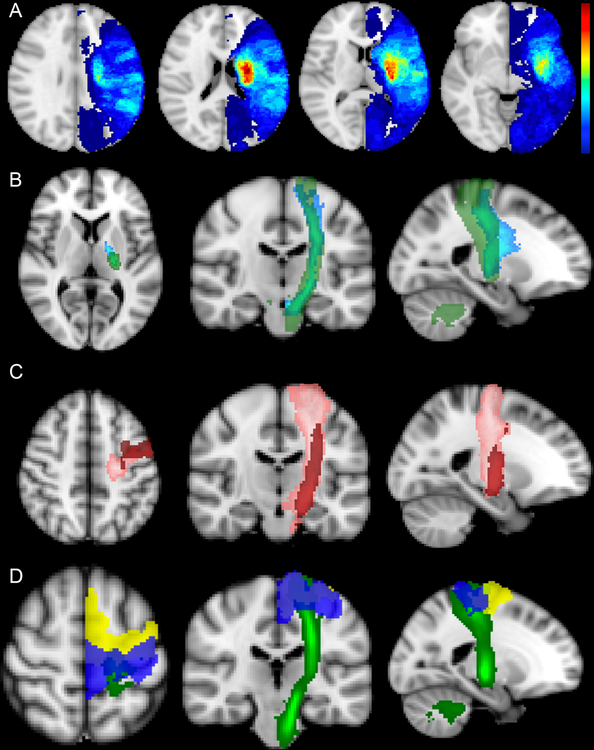
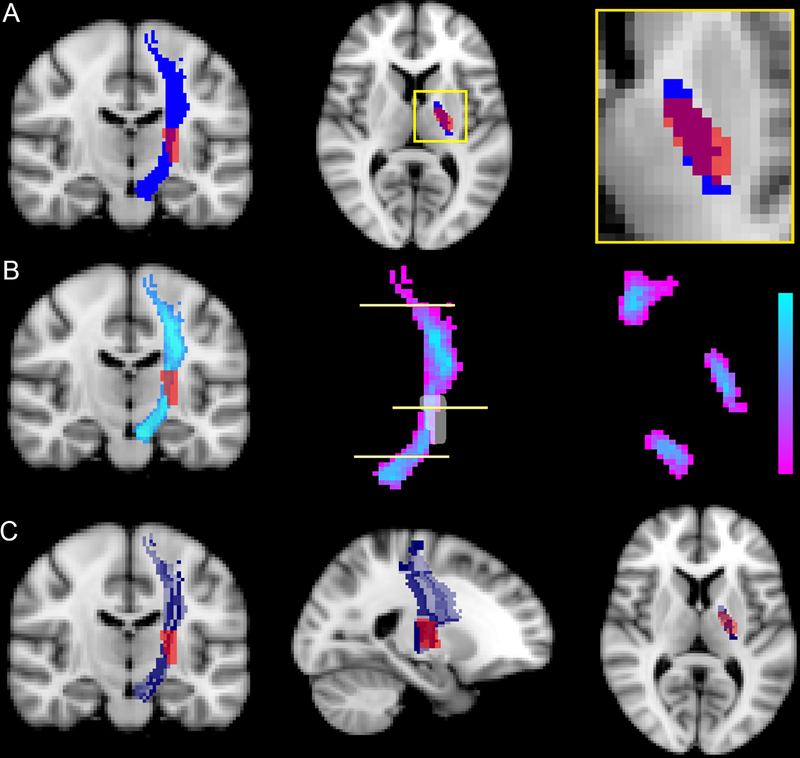
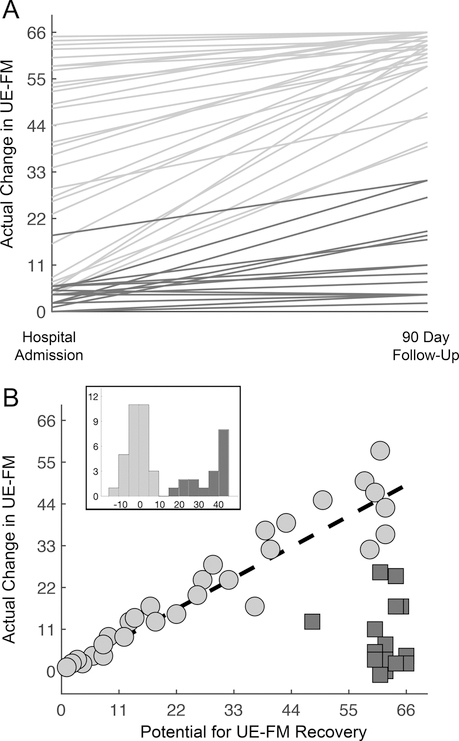
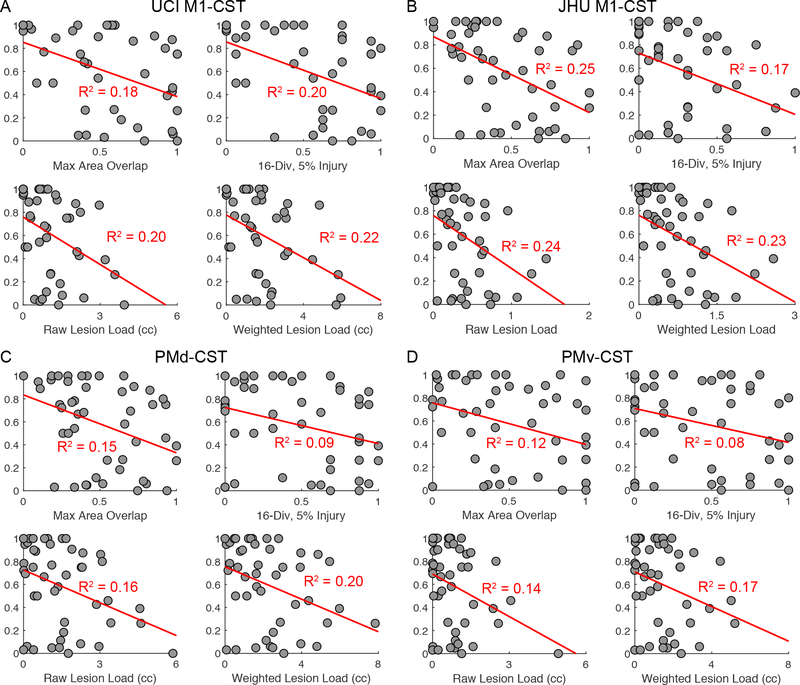
Background and Purpose- Injury to the corticospinal tract (CST) has been shown to have a major effect on upper extremity motor recovery after stroke. This study aimed to examine how well CST injury, measured from neuroimaging acquired during the acute stroke workup, predicts upper extremity motor recovery. Methods- Patients with upper extremity weakness after ischemic stroke were assessed using the upper extremity Fugl-Meyer during the acute stroke hospitalization and again at 3-month follow-up. CST injury was quantified and compared, using 4 different methods, from images obtained as part of the stroke standard-of-care workup. Logistic and linear regression were performed using CST injury to predict ΔFugl-Meyer. Injury to primary motor and premotor cortices were included as potential modifiers of the effect of CST injury on recovery. Results- N=48 patients were enrolled 4.2±2.7 days poststroke and completed 3-month follow-up (median 90-day modified Rankin Scale score, 3; interquartile range, 1.5). CST injury distinguished patients who reached their recovery potential (as predicted from initial impairment) from those who did not, with area under the curve values ranging from 0.70 to 0.8. In addition, CST injury explained ≈20% of the variance in the magnitude of upper extremity recovery, even after controlling for the severity of initial impairment. Results were consistent when comparing 4 different methods of measuring CST injury. Extent of injury to primary motor and premotor cortices did not significantly influence the predictive value that CST injury had for recovery. Conclusions- Structural injury to the CST, as estimated from standard-of-care imaging available during the acute stroke hospitalization, is a robust way to distinguish patients who achieve their predicted recovery potential and explains a significant amount of the variance in poststroke upper extremity motor recovery.
Keywords: area under curve; humans; neuroimaging; neurological rehabilitation; pyramidal tracts.
Figures
References
-
- Langhorne P, Coupar F, Pollock A. Motor recovery after stroke: A systematic review. Lancet Neurol 2009;8:741–754 - PubMed
-
- Kwakkel G, Kollen B, Twisk J. Impact of time on improvement of outcome after stroke. Stroke. 2006;37:2348–2353 - PubMed
-
- Duncan PW, Goldstein LB, Matchar D, Divine GW, Feussner J. Measurement of motor recovery after stroke. Outcome assessment and sample size requirements. Stroke. 1992;23:1084–1089 - PubMed
-
- Prabhakaran S, Zarahn E, Riley C, Speizer A, Chong JY, Lazar RM, et al. Inter-individual variability in the capacity for motor recovery after ischemic stroke. Neurorehabil Neural Repair. 2008;22:64–71 - PubMed
-
- Winters C, van Wegen EE, Daffertshofer A, Kwakkel G. Generalizability of the proportional recovery model for the upper extremity after an ischemic stroke. Neurorehabil Neural Repair. 2015;29:614–622 - PubMed
