

Comparison of the Hemodynamic Response to Intra-Aortic Balloon Counterpulsation in Patients With Cardiogenic Shock Resulting from Acute Myocardial Infarction Versus Acute Decompensated Heart Failure
- PMID: 31648782
- PMCID: PMC6937209
- DOI: 10.1016/j.amjcard.2019.09.016
Comparison of the Hemodynamic Response to Intra-Aortic Balloon Counterpulsation in Patients With Cardiogenic Shock Resulting from Acute Myocardial Infarction Versus Acute Decompensated Heart Failure
Abstract
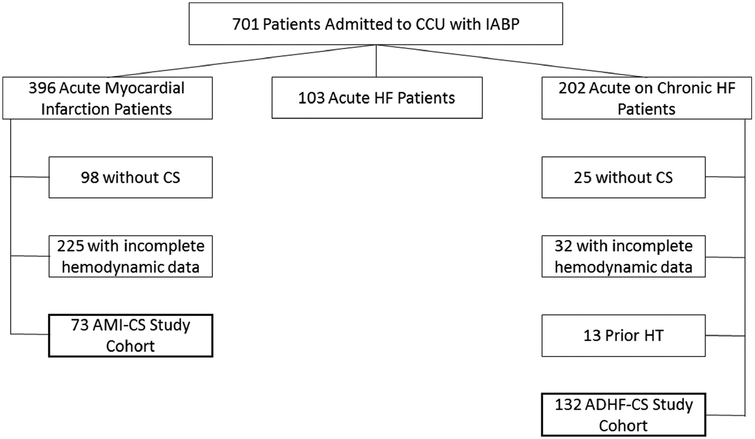
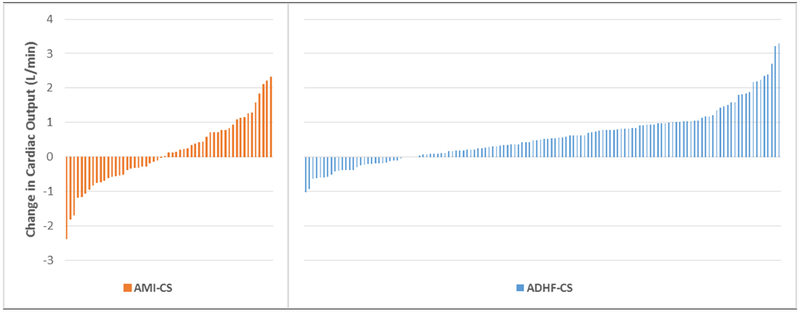
The intra-aortic balloon pump (IABP) neither benefits nor harms patients with acute myocardial infarction (AMI) with cardiogenic shock (CS) but may stabilize those with chronic heart failure who decompensate into CS. We sought to compare its hemodynamic effects in these 2 populations. We performed a retrospective analysis of the hemodynamic effects of IABP for AMI or acute decompensated heart failure (ADHF) patients with hemodynamic evidence of CS. The primary outcome was cardiac output (CO) change following insertion. In total, 205 patients were treated for CS resulting from AMI (73; 35.6%) or ADHF (132; 64.4%). At baseline, both cohorts had significant hemodynamic compromise with mean arterial pressure 75.6 ± 12.3 mm Hg, CO 3.02 ± 0.84 L/min, and cardiac power index 0.26 ± 0.06 W/m2; these parameters were nearly identical between groups though ADHF-CS patients had a higher pre-IABP mean pulmonary artery (PA) pressure than AMI-CS patients. After IABP insertion, ADHF-CS patients had moderate CO augmentation whereas AMI-CS experienced almost no improvement (0.58 ± 0.79 L/min vs 0.12 ± 1.00 L/min; p = 0.0009). Intracardiac filling pressures were reduced by similar amounts in both cohorts. Systemic vascular resistance was reduced in patients with ADHF-CS but not in those with AMI-CS. In conclusion, following IABP insertion, ADHF-CS patients experience roughly a 5-fold greater CO augmentation compared with AMI-CS patients. Pre-IABP PA pressure differences and differential systemic vascular resistance reduction may explain these results and shed light on recent evidence supporting IABP use in ADHF-CS and curbing it in AMI-CS.
Copyright © 2019 Elsevier Inc. All rights reserved.
Figures
References
-
- Goldberg RJ, Makam RC, Yarzebski J, McManus DD, Lessard D, Gore JM. Decade-long trends (2001-2011) in the Incidence and Hospital Death Rates Associated with the In-Hospital Development of Cardiogenic Shock after Acute Myocardial Infarction. Circ Cardiovasc Qual Outcomes 2016;9:117–125. - PMC - PubMed
-
- Werdan K, Gielen S, Ebelt H, Hochman JS. Mechanical circulatory support in cardiogenic shock. Eur Heart J 2014; 35:156–167. - PubMed
-
- Stretch R, Sauer CM, Yuh DD, Bonde P. National trends in the utilization of short-term mechanical circulatory support: incidence, outcomes, and cost analysis. J Am Coll Cardiol 2014;64:407–415. - PubMed
-
- Fried JA, Nair A, Takeda K, Clerkin K, Topkara VK, Masoumi A, Yuzefpolskaya M, Takayama H, Naka Y, Burkhoff D, Kirtane A, Karmpaliotis D, Moses J, Colombo PC, Garan AR. Clinical and Hemodynamic Effects of Intra-Aortic Balloon Pump Therapy in Chronic Heart Failure Patients with Cardiogenic Shock. J Heart Lung Transplant 2018;37:1313–1321. - PMC - PubMed
-
- Sintek MA, Gdowski M, Lindman BR, Nassif M, Lavine KJ, Novak E, Bach RG, Silvestry SC, Mann DL, Joseph SM. Intra-aortic balloon counterpulsation in patients with chronic heart failure and cardiogenic shock: Clinical Response and Predictors of Stabilization. J Card Fail 2015;21:868–876. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
