

Clinical Utility of the Nuclear-localized AR-V7 Biomarker in Circulating Tumor Cells in Improving Physician Treatment Choice in Castration-resistant Prostate Cancer
- PMID: 31648903
- PMCID: PMC7472426
- DOI: 10.1016/j.eururo.2019.08.020
Clinical Utility of the Nuclear-localized AR-V7 Biomarker in Circulating Tumor Cells in Improving Physician Treatment Choice in Castration-resistant Prostate Cancer
Abstract
Background: Proof of the clinical utility of a biomarker is when its use informs a management decision and improves patient outcomes relative to when it is not used.
Objective: To model the clinical benefit of the nuclear-localized androgen receptor splice variant 7 (AR-V7) test for men with progressing metastatic castration-resistant prostate cancer (mCRPC) at the second line of therapy or greater to inform the choice of an androgen receptor signaling inhibitor (ARSI) or a taxane.
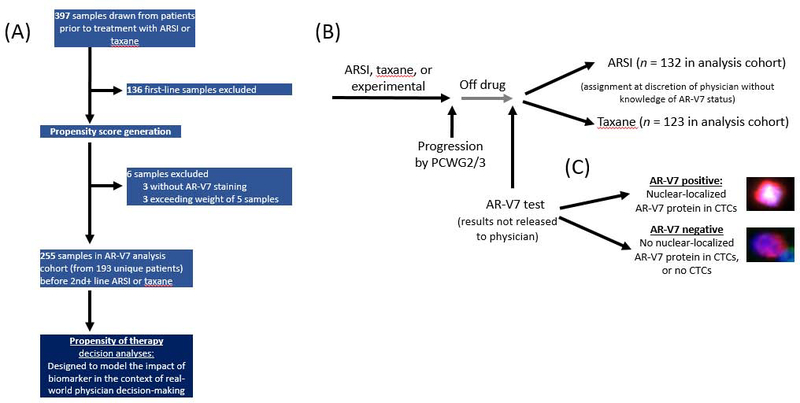
Design, setting, and participants: The study population was a cross-sectional cohort of 193 unique patients with progressing mCRPC from whom 255 samples were drawn at the time of the second line or later treatment decision who then received an ARSI or taxane, with up to 3 yr of additional follow-up Circulating tumor cells (CTCs) were identified from blood samples and tested for AR-V7. Physicians were blinded to AR-V7 status and the testing laboratory was blinded to outcomes.
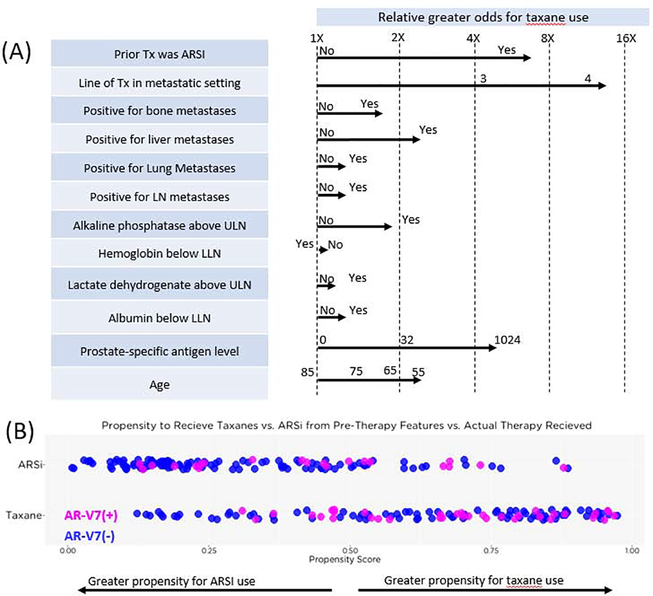
Outcome measurements and statistical analyses: We measured physician propensity for choosing an ARSI or taxane based on patient prognosis. We also measured overall survival (OS) adjusted for physician propensity by drug class; OS data were analyzed both without and with knowledge of nuclear-localized AR-V7 status.
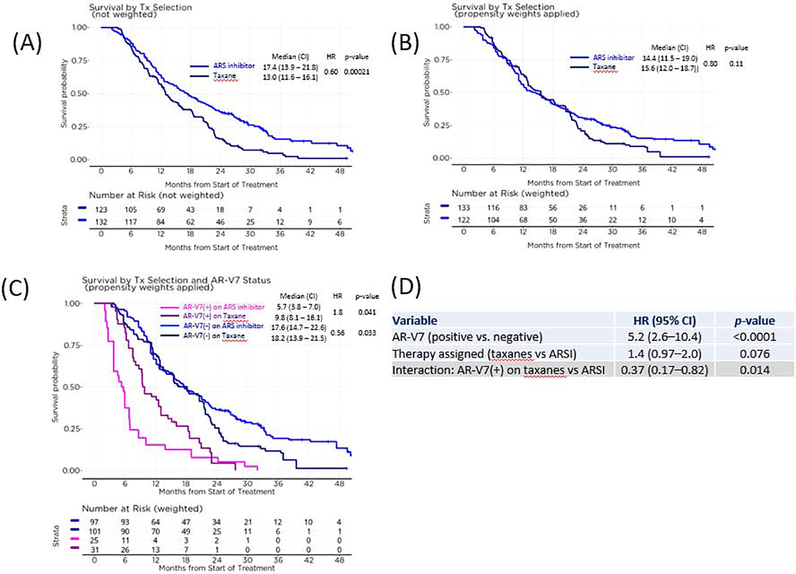
Results and limitations: Treating physicians had a propensity for choosing a taxane over an ARSI for patients with more advanced disease or who received an ARSI as the immediate prior therapy. After adjusting for physician propensity, discernible OS differences were not observed between taxane- and ARSI-treated patients (median 15.6 vs 14.4 mo; p =0.11). Patients with detectable nuclear-localized AR-V7 in CTCs had superior survival with taxanes over ARSIs (median 9.8 vs 5.7 mo; p = 0.041). AR-V7-negative patients had superior survival on ARSIs over taxanes (p = 0.033) but overlapping curves limit the interpretation. Mutivariable models showed a robust interaction between AR-V7 status and drug, and a lower risk of death on taxanes for AR-V7-positive men.
Conclusions: Use of the nuclear-localized AR-V7 CTC test to inform treatment choice can improve patient outcomes relative to decisions based solely on standard-of-care measures.
Patient summary: Men with metastatic prostate cancer who test positive for AR-V7 protein in circulating tumor cells are likely to live longer if taxane chemotherapy is used.
Keywords: AR-V7; Circulating tumor cells; Liquid biopsy; Prostate cancer; Treatment decisions.
Copyright © 2019. Published by Elsevier B.V.
Figures
Comment in
-
Clinical Acumen Versus Androgen Receptor Variant 7 Circulating Tumor Cells in Decision-Making for Men with Advanced Prostate Cancer.Eur Urol. 2020 Feb;77(2):178-179. doi: 10.1016/j.eururo.2019.09.028. Epub 2019 Oct 13. Eur Urol. 2020. PMID: 31615710 No abstract available.
-
Clinical decision-making with AR-V7.Nat Rev Urol. 2019 Dec;16(12):694. doi: 10.1038/s41585-019-0259-2. Nat Rev Urol. 2019. PMID: 31690843 No abstract available.
-
Clinical utility of the nuclear-localized AR-V7 biomarker for treatment choice in metastatic castration-resistant prostate cancer.Transl Androl Urol. 2020 Dec;9(6):2483-2487. doi: 10.21037/tau-20-968. Transl Androl Urol. 2020. PMID: 33457221 Free PMC article. No abstract available.
References
-
- Ryan CJ, Smith MR, Fizazi K, et al. Abiraterone acetate plus prednisone versus placebo plus prednisone in chemotherapy-naive men with metastatic castration-resistant prostate cancer (COU-AA-302): final overall survival analysis of a randomised, double-blind, placebo-controlled phase 3 study. Lancet Oncol 2015;16:152–60. - PubMed
-
- Schrader AJ, Boegemann M, Ohlmann CH, et al. Enzalutamide in castration-resistant prostate cancer patients progressing after docetaxel and abiraterone. Eur Urol 2014;65:30–6. - PubMed
-
- Azad AA, Eigl BJ, Murray RN, Kollmannsberger C, Chi KN. Efficacy of enzalutamide following abiraterone acetate in chemotherapy-naive metastatic castration-resistant prostate cancer patients. Eur Urol 2015;67:23–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
