

Financial impact of improving patient care setting selection after bariatric surgery
- PMID: 31648980
- PMCID: PMC6941883
- DOI: 10.1016/j.soard.2019.06.029
Financial impact of improving patient care setting selection after bariatric surgery
Abstract
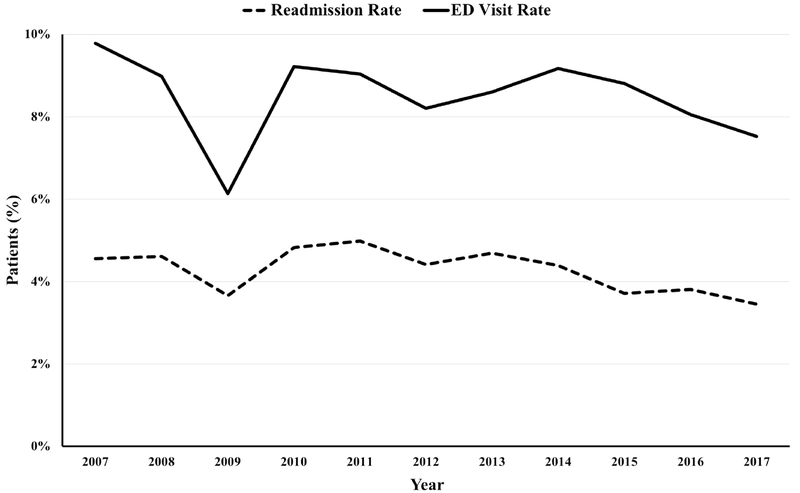
Background: Potentially avoidable emergency department (ED) visits are a significant source of excess healthcare spending. Despite improvement in postoperative readmissions, 20% of bariatric surgery patients use the ED postoperatively. Many of these visits may be appropriately managed in lower-acuity centers.
Objective: We sought to evaluate the economic impact of shifting potentially avoidable ED visits after bariatric surgery to lower-acuity centers.
Setting: Statewide quality improvement collaborative.
Methods: We performed an observational study of patients who underwent bariatric surgery between 2011 and 2017 using a linked data registry, including clinical data from a large-quality improvement collaborative and payment data from a statewide value collaborative. Postoperative ED visits and readmission rates were determined. Ninety-day ED and urgent care center (UCC) visit claims were matched to a clinical registry. Price-standardized payments for UCC and ED visits without admission were compared.
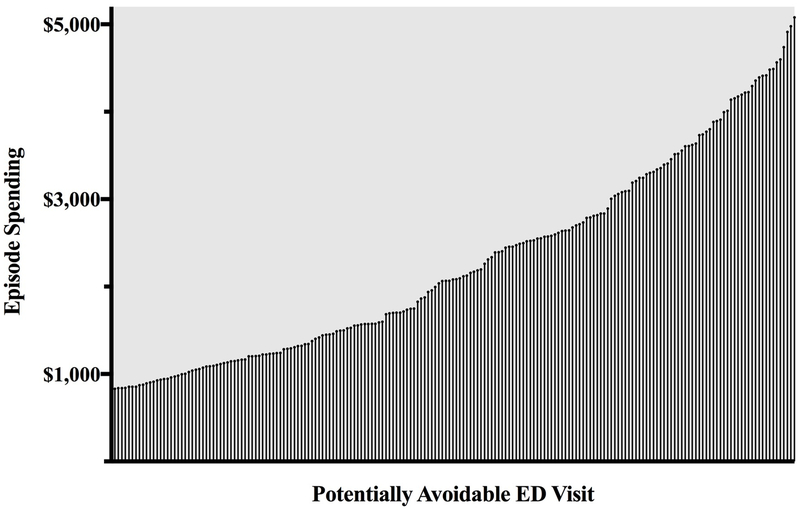
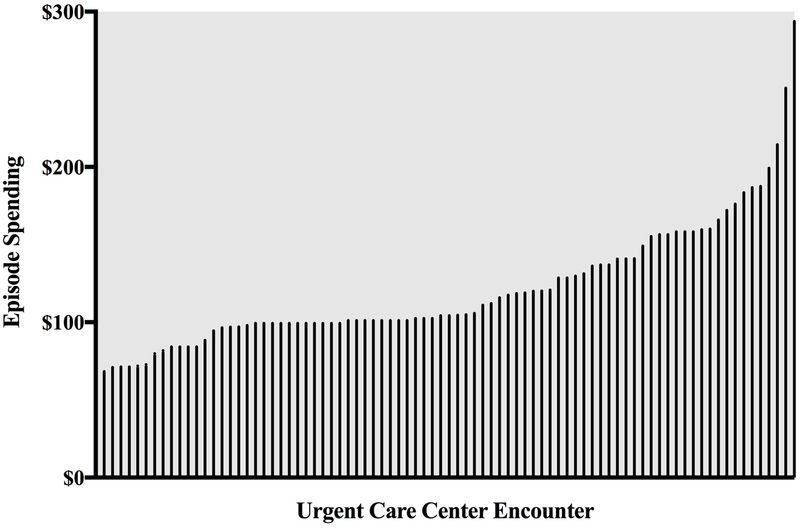
Results: Among the 36,071 patients who underwent bariatric surgery, 8.4% presented to the ED postoperatively. Approximately 50% of these visits resulted in readmission. Three hundred eighty-eight ED visits without readmission (i.e., potentially avoidable ED visits) and 110 UCC encounters with claims data were identified. Triaging a potentially avoidable ED visit to an UCC would generate a savings of $4238 per patient, reducing spending in this cohort by $1.6 million.
Conclusion: Shifting potentially avoidable ED visits after bariatric surgery could result in significant cost savings. Efforts to improve patients' selection of healthcare setting and increase utilization of lower-acuity centers may serve as a template for appropriately meeting the needs of patients and containing spending after bariatric surgery.
Keywords: Bariatric surgery; Cost containment; Emergency department visit; Health policy; Nonurgent ED visit; Urgent care center.
Copyright © 2019 American Society for Bariatric Surgery. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Metabolic and Bariatric Surgery Accreditation and Quality Improvement Program. https://www.facs.org/quality-programs/mbsaqip. Accessed March 19, 2018.
-
- Abraham CR, Werter CR, Ata A, et al. Predictors of Hospital Readmission after Bariatric Surgery. J Am Coll Surg. 2015;221(1):220–227. - PubMed
-
- Encinosa WE, Bernard DM, Du D, Steiner CA. Recent improvements in bariatric surgery outcomes. Med Care. 2009;47(5):531–535. - PubMed
-
- Mora-Pinzon MC, Henkel D, Miller RE, et al. Emergency department visits and readmissions within 1 year of bariatric surgery: A statewide analysis using hospital discharge records. Surgery. 2017;162(5):1155–1162. - PubMed
-
- Morton J The first metabolic and bariatric surgery accreditation and quality improvement program quality initiative: decreasing readmissions through opportunities provided. Surg Obes Relat Dis. 2014;10(3):377–378. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
