

Exploration of surgical blood pressure management and expected motor recovery in individuals with traumatic spinal cord injury
- PMID: 31649323
- PMCID: PMC7062632
- DOI: 10.1038/s41393-019-0370-5
Exploration of surgical blood pressure management and expected motor recovery in individuals with traumatic spinal cord injury
Erratum in
-
Correction: Exploration of surgical blood pressure management and expected motor recovery in individuals with traumatic spinal cord injury.Spinal Cord. 2020 Mar;58(3):387. doi: 10.1038/s41393-019-0400-3. Spinal Cord. 2020. PMID: 31822809 Free PMC article.
-
Correction: Exploration of surgical blood pressure management and expected motor recovery in individuals with traumatic spinal cord injury.Spinal Cord. 2020 Aug;58(8):943-945. doi: 10.1038/s41393-020-0504-9. Spinal Cord. 2020. PMID: 32576945 Free PMC article.
Abstract
Study design: Retrospective analysis.
Objective: To assess the impact of mean arterial blood pressure (MAP) during surgical intervention for spinal cord injury (SCI) on motor recovery.
Setting: Level-one Trauma Hospital and Acute Rehabilitation Hospital in San Jose, CA, USA.
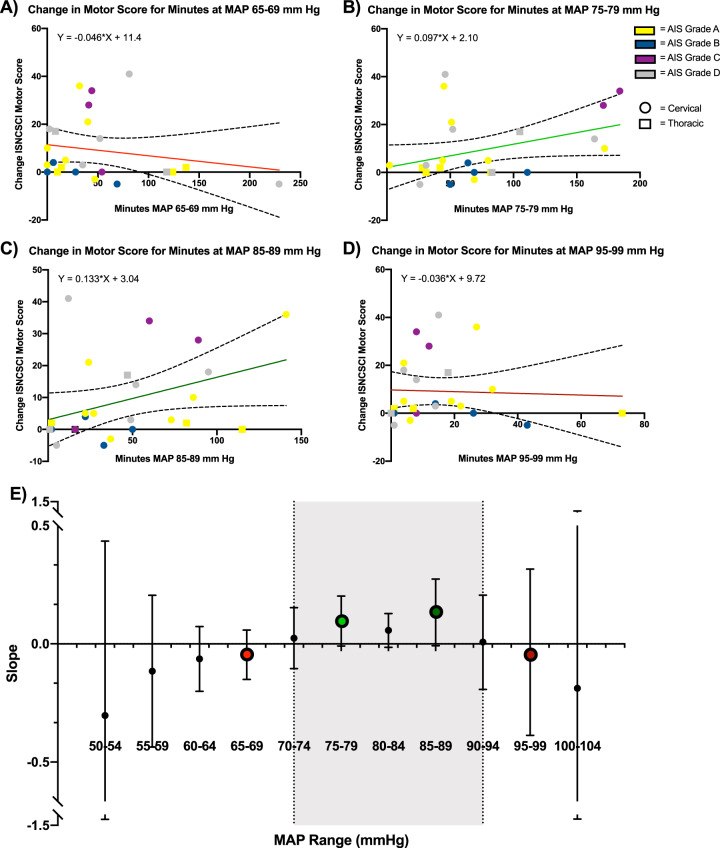
Methods: Twenty-five individuals with traumatic SCI who received surgical and acute rehabilitation care at a level-one trauma center were included in this study. The Surgical Information System captured intraoperative MAPs on a minute-by-minute basis and exposure was quantified at sequential thresholds from 50 to 104 mmHg. Change in International Standards for Neurological Classification of Spinal Cord Injury (ISNCSCI) motor score was calculated based on physiatry evaluations at the earliest postoperative time and at discharge from acute rehabilitation. Linear regression models were used to estimate the rate of recovery across the entire MAP range.
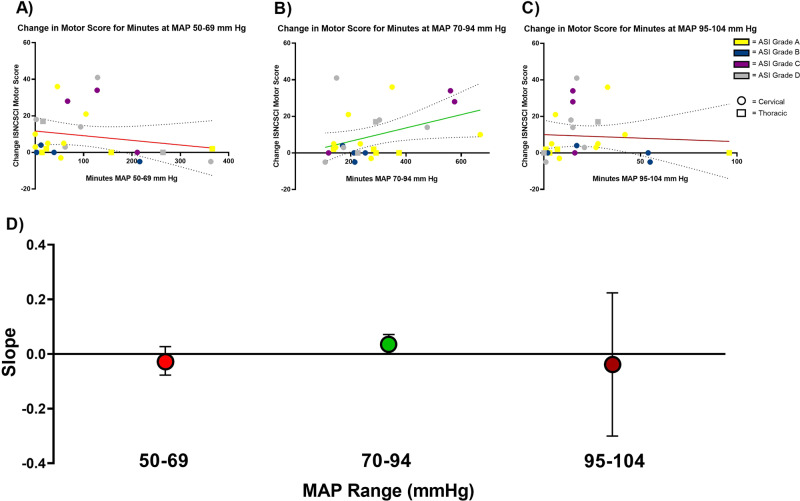
Results: An exploratory analysis revealed that increased time within an intraoperative MAP range (70-94 mmHg) was associated with ISNCSCI motor score improvement. A significant regression equation was found for the MAP range 70-94 mmHg (F[1, 23] = 5.07, r2 = 0.181, p = 0.034). ISNCSCI motor scores increased 0.039 for each minute of exposure to the MAP range 70-94 mmHg during the operative procedure; this represents a significant correlation between intraoperative time with MAP 70-94 and subsequent motor recovery. Blood pressure exposures above or below this range did not display a positive association with motor recovery.
Conclusions: Hypertension as well as hypotension during surgery may impact the trajectory of recovery in individuals with SCI, and there may be a direct relationship between intraoperative MAP and motor recovery.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
-
- Spinal cord injury [Internet]. World Health Organization. 2013 [cited 2019 Aug 30]. https://www.who.int/news-room/fact-sheets/detail/spinal-cord-injury.
-
- National Spinal Cord Injury Statistical Center. Facts and figures at a glance. Birmingham, AL: University of Alabama at Birmingham; 2018.
