

Incidence trends and survival prediction of hepatoblastoma in children: a population-based study
- PMID: 31651371
- PMCID: PMC6813130
- DOI: 10.1186/s40880-019-0411-7
Incidence trends and survival prediction of hepatoblastoma in children: a population-based study
Abstract
Background: Hepatoblastoma is a rare disease that nevertheless accounts for the majority of liver malignancies in children. Due to limited epidemiological data, therapy for hepatoblastoma tends to be individualized. This study aimed to evaluate incidence trends of hepatoblastoma and to develop a nomogram to predict the survival of children with newly diagnosed hepatoblastoma on a population-based level.
Methods: Individuals up to 18 years of age with hepatoblastoma recorded in 18 registries of the Surveillance, Epidemiology, and End Results (SEER) database between 2004 and 2015 were examined. Joinpoint regression analyses were applied to assess incidence trends in annual percentage change (APC). Multivariable Cox regression was used to identify factors associated with overall survival (OS). A nomogram was constructed to predict OS in individual cases based on independent predictors. Concordance index (C-index) and calibration curves were used to evaluate predictive performance.
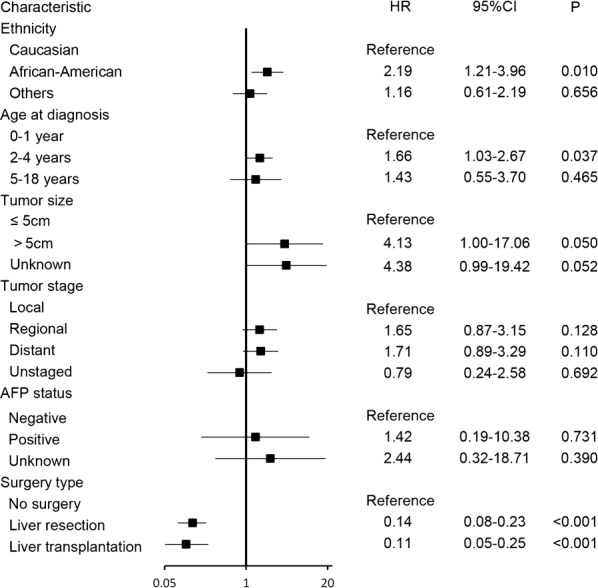
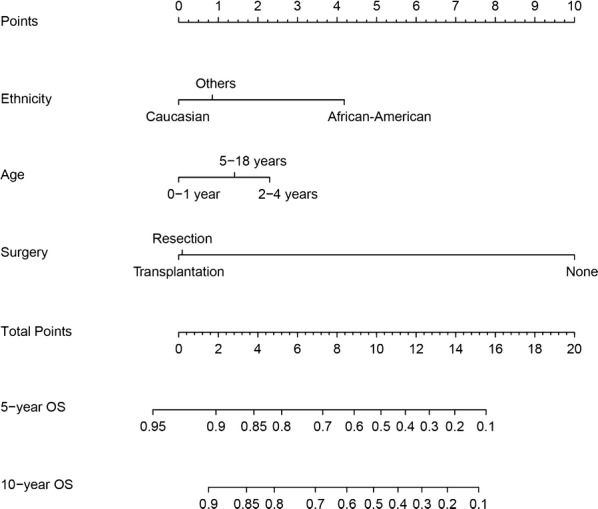
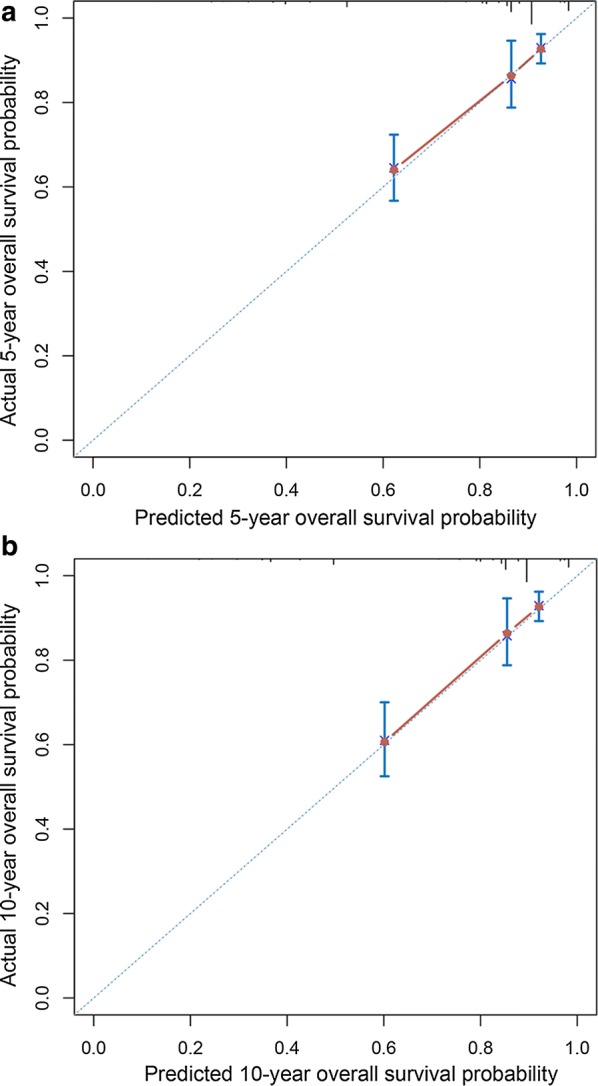
Results: Between 2004 and 2015, hepatoblastoma incidence increased significantly (APC, 2.2%; 95% confidence interval [CI] 0.5% to 3.8%, P < 0.05). In particular, this increase was observed among 2- to 4-year-old patients, males, and African-Americans. The 5- and 10-year OS rates were 81.5% and 81.0%, respectively. Age of 2 to 4 years, African-American ethnicity, and no surgery were independent predictors for short OS. Distant disease at presentation was found not to be an independent factor of survival. The nomogram had a C-index of 0.79 (95% CI 0.74-0.84) with appropriate calibration curve fitting.
Conclusions: We constructed a nomogram that integrates common factors associated with survival for hepatoblastoma patients. It provides accurate prognostic prediction for children with hepatoblastoma.
Keywords: Hepatoblastoma; Incidence; Liver surgery; Liver transplantation; Nomogram; Overall survival; Pediatric surgery; SEER.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
-
- Darbari A, Sabin KM, Shapiro CN, Schwarz KB. Epidemiology of primary hepatic malignancies in U.S. children. Hepatology. 2003;38(3):560–566. - PubMed
-
- Meyers RL. Tumors of the liver in children. Surg Oncol. 2007;16(3):195–203. - PubMed
-
- Finegold MJ, Egler RA, Goss JA, Guillerman RP, Karpen SJ, Krishnamurthy R, et al. Liver tumors: pediatric population. Liver Transpl. 2008;14(11):1545–1556. - PubMed
-
- Litten JB, Tomlinson GE. Liver tumors in children. Oncologist. 2008;13(7):812–820. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
