

Randomized Trial of Lenalidomide Versus Observation in Smoldering Multiple Myeloma
- PMID: 31652094
- PMCID: PMC7145586
- DOI: 10.1200/JCO.19.01740
Randomized Trial of Lenalidomide Versus Observation in Smoldering Multiple Myeloma
Abstract
Purpose: Observation is the current standard of care for smoldering multiple myeloma. We hypothesized that early intervention with lenalidomide could delay progression to symptomatic multiple myeloma.
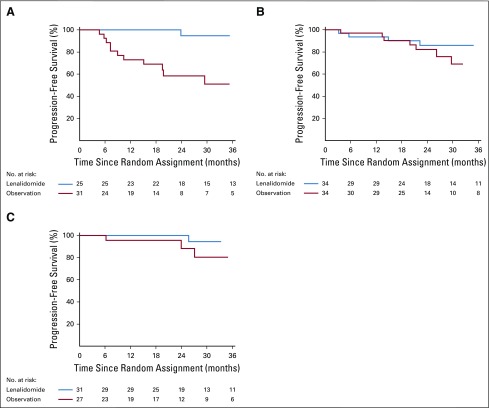
Methods: We conducted a randomized trial that assessed the efficacy of single-agent lenalidomide compared with observation in patients with intermediate- or high-risk smoldering multiple myeloma. Lenalidomide was administered orally at a dose of 25 mg on days 1 to 21 of a 28-day cycle. The primary end point was progression-free survival, with disease progression requiring the development of end-organ damage attributable to multiple myeloma and biochemical progression.
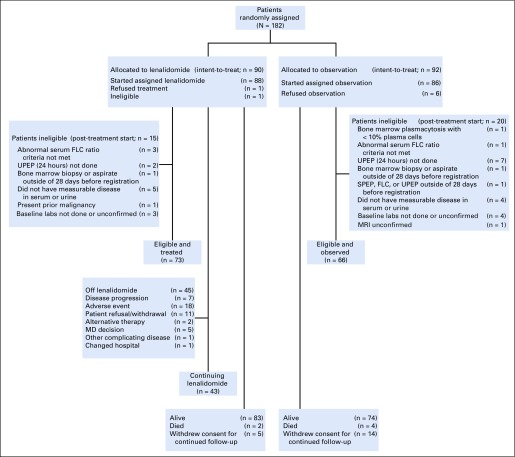
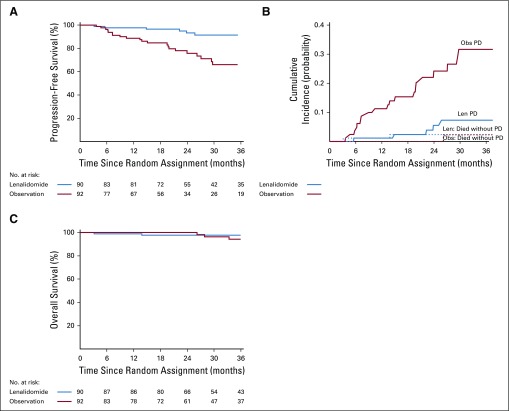
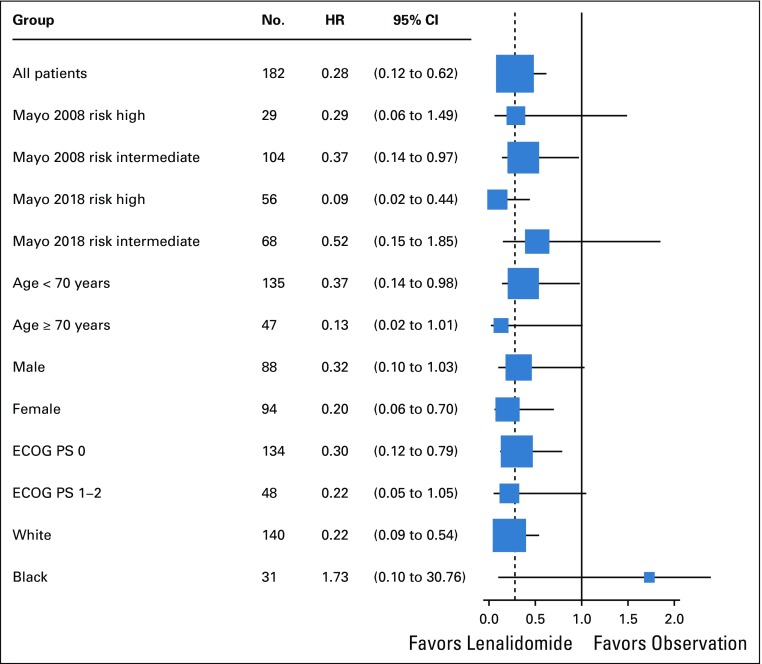
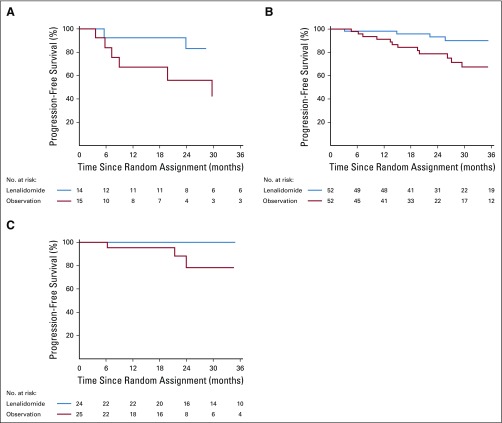
Results: One hundred eighty-two patients were randomly assigned-92 patients to the lenalidomide arm and 90 to the observation arm. Median follow-up is 35 months. Response to therapy was observed in 50% (95% CI, 39% to 61%) of patients in the lenalidomide arm, with no responses in the observation arm. Progression-free survival was significantly longer with lenalidomide compared with observation (hazard ratio, 0.28; 95% CI, 0.12 to 0.62; P = .002). One-, 2-, and 3-year progression-free survival was 98%, 93%, and 91% for the lenalidomide arm versus 89%, 76%, and 66% for the observation arm, respectively. Only six deaths have been reported, two in the lenalidomide arm versus four in the observation arm (hazard ratio for death, 0.46; 95% CI, 0.08 to 2.53). Grade 3 or 4 nonhematologic adverse events occurred in 25 patients (28%) on lenalidomide.
Conclusion: Early intervention with lenalidomide in smoldering multiple myeloma significantly delays progression to symptomatic multiple myeloma and the development of end-organ damage.
Trial registration: ClinicalTrials.gov NCT01169337.
Figures




Comment in
-
How We Approach Smoldering Multiple Myeloma.J Clin Oncol. 2020 Apr 10;38(11):1119-1125. doi: 10.1200/JCO.19.02834. Epub 2020 Jan 31. J Clin Oncol. 2020. PMID: 32004107 Free PMC article.
-
Reply to N. Biran et al.J Clin Oncol. 2020 Apr 20;38(12):1368-1369. doi: 10.1200/JCO.20.00042. Epub 2020 Mar 11. J Clin Oncol. 2020. PMID: 32160076 No abstract available.
-
Treatment of Smoldering Myeloma: Problems With Study Design as well as Biological and Clinical Implications.J Clin Oncol. 2020 Apr 20;38(12):1367-1368. doi: 10.1200/JCO.19.02972. Epub 2020 Mar 11. J Clin Oncol. 2020. PMID: 32160077 No abstract available.
References
-
- Rajkumar SV, Dimopoulos MA, Palumbo A, et al. International Myeloma Working Group updated criteria for the diagnosis of multiple myeloma. Lancet Oncol. 2014;15:e538–e548. - PubMed
-
- Kyle RA, Remstein ED, Therneau TM, et al. Clinical course and prognosis of smoldering (asymptomatic) multiple myeloma. N Engl J Med. 2007;356:2582–2590. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- U10 CA180826/CA/NCI NIH HHS/United States
- P30 CA016672/CA/NCI NIH HHS/United States
- UG1 CA189870/CA/NCI NIH HHS/United States
- UL1 TR001863/TR/NCATS NIH HHS/United States
- UG1 CA189805/CA/NCI NIH HHS/United States
- U10 CA180858/CA/NCI NIH HHS/United States
- R01 CA168762/CA/NCI NIH HHS/United States
- P50 CA186781/CA/NCI NIH HHS/United States
- UG1 CA189828/CA/NCI NIH HHS/United States
- UG1 CA189863/CA/NCI NIH HHS/United States
- U10 CA180790/CA/NCI NIH HHS/United States
- U10 CA180820/CA/NCI NIH HHS/United States
- U10 CA180794/CA/NCI NIH HHS/United States
- U10 CA180888/CA/NCI NIH HHS/United States
- U10 CA180853/CA/NCI NIH HHS/United States
- U10 CA180864/CA/NCI NIH HHS/United States
- R35 CA197603/CA/NCI NIH HHS/United States
- R01 CA107476/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
