

Myeloid-Derived Suppressor Cells and Pancreatic Cancer: Implications in Novel Therapeutic Approaches
- PMID: 31652904
- PMCID: PMC6893814
- DOI: 10.3390/cancers11111627
Myeloid-Derived Suppressor Cells and Pancreatic Cancer: Implications in Novel Therapeutic Approaches
Abstract
Pancreatic ductal adenocarcinoma (PDAC) remains a devastating human malignancy with poor prognosis and low survival rates. Several cellular mechanisms have been linked with pancreatic carcinogenesis and also implicated in inducing tumor resistance to known therapeutic regimens. Of various factors, immune evasion mechanisms play critical roles in tumor progression and impeding the efficacy of cancer therapies including PDAC. Among immunosuppressive cell types, myeloid-derived suppressor cells (MDSCs) have been extensively studied and demonstrated to not only support PDAC development but also hamper the anti-tumor immune responses elicited by therapeutic agents. Notably, recent efforts have been directed in devising novel approaches to target MDSCs to limit their effects. Multiple strategies including immune-based approaches have been explored either alone or in combination with therapeutic agents to target MDSCs in preclinical and clinical settings of PDAC. The current review highlights the roles and mechanisms of MDSCs as well as the implications of this immunomodulatory cell type as a potential target to improve the efficacy of therapeutic regimens for PDAC.
Keywords: myeloid-derived suppressor cells; pancreatic cancer; pancreatic cancer therapies.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
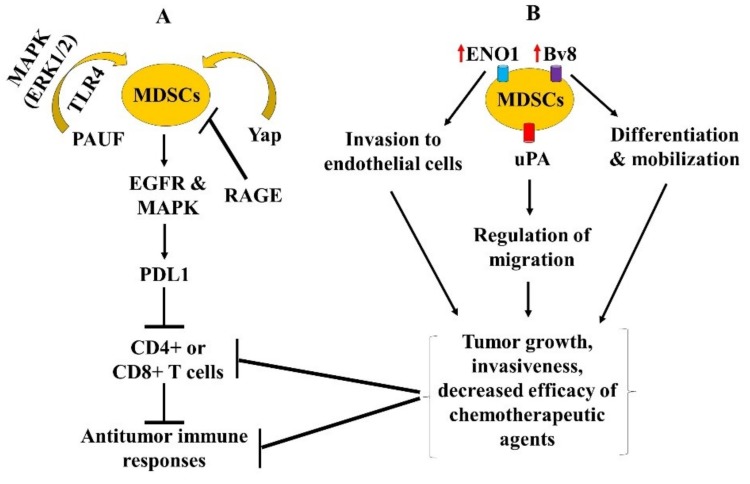
 inhibition and
inhibition and  increase or upregulation.
increase or upregulation.Similar articles
-
Myeloid-Derived Suppressor Cells: A New and Pivotal Player in Colorectal Cancer Progression.Front Oncol. 2020 Dec 15;10:610104. doi: 10.3389/fonc.2020.610104. eCollection 2020. Front Oncol. 2020. PMID: 33384962 Free PMC article. Review.
-
CD13hi Neutrophil-like myeloid-derived suppressor cells exert immune suppression through Arginase 1 expression in pancreatic ductal adenocarcinoma.Oncoimmunology. 2017 Jan 9;6(2):e1258504. doi: 10.1080/2162402X.2016.1258504. eCollection 2017. Oncoimmunology. 2017. PMID: 28344866 Free PMC article.
-
Murine- and Human-Derived Autologous Organoid/Immune Cell Co-Cultures as Pre-Clinical Models of Pancreatic Ductal Adenocarcinoma.Cancers (Basel). 2020 Dec 17;12(12):3816. doi: 10.3390/cancers12123816. Cancers (Basel). 2020. PMID: 33348809 Free PMC article.
-
The role of 2-arachidonoylglycerol in the regulation of the tumor-immune microenvironment in murine models of pancreatic cancer.Biomed Pharmacother. 2019 Jul;115:108952. doi: 10.1016/j.biopha.2019.108952. Epub 2019 May 9. Biomed Pharmacother. 2019. PMID: 31078044
-
Myeloid-derived suppressor cells: The green light for myeloma immune escape.Blood Rev. 2016 Sep;30(5):341-8. doi: 10.1016/j.blre.2016.04.002. Epub 2016 Apr 12. Blood Rev. 2016. PMID: 27132116 Free PMC article. Review.
Cited by
-
The Latest Advancement in Pancreatic Ductal Adenocarcinoma Therapy: A Review Article for the Latest Guidelines and Novel Therapies.Biomedicines. 2021 Apr 6;9(4):389. doi: 10.3390/biomedicines9040389. Biomedicines. 2021. PMID: 33917380 Free PMC article. Review.
-
Spatial genomics reveals a high number and specific location of B cells in the pancreatic ductal adenocarcinoma microenvironment of long-term survivors.Front Immunol. 2023 Jan 4;13:995715. doi: 10.3389/fimmu.2022.995715. eCollection 2022. Front Immunol. 2023. PMID: 36685537 Free PMC article.
-
Apigenin Targets MicroRNA-155, Enhances SHIP-1 Expression, and Augments Anti-Tumor Responses in Pancreatic Cancer.Cancers (Basel). 2022 Jul 25;14(15):3613. doi: 10.3390/cancers14153613. Cancers (Basel). 2022. PMID: 35892872 Free PMC article.
-
Overcoming the Fibrotic Fortress in Pancreatic Ductal Adenocarcinoma: Challenges and Opportunities.Cancers (Basel). 2023 Apr 18;15(8):2354. doi: 10.3390/cancers15082354. Cancers (Basel). 2023. PMID: 37190281 Free PMC article. Review.
-
Protein Signature Differentiating Neutrophils and Myeloid-Derived Suppressor Cells Determined Using a Human Isogenic Cell Line Model and Protein Profiling.Cells. 2024 May 7;13(10):795. doi: 10.3390/cells13100795. Cells. 2024. PMID: 38786019 Free PMC article.
References
-
- Pal S.K., Miller M.J., Agarwal N., Chang S.M., Chavez-MacGregor M., Cohen E., Cole S., Dale W., Magid Diefenbach C.S., Disis M.L., et al. Clinical cancer advances 2019: Annual report on progress against cancer from the American Society of Clinical Oncology. J. Clin. Oncol. 2019;37:834–849. doi: 10.1200/JCO.18.02037. - DOI - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
