

Systolic blood pressure as a predictor of transient ischemic attack/minor stroke in emergency department patients under age 80: a prospective cohort study
- PMID: 31653207
- PMCID: PMC6815025
- DOI: 10.1186/s12883-019-1466-4
Systolic blood pressure as a predictor of transient ischemic attack/minor stroke in emergency department patients under age 80: a prospective cohort study
Abstract
Background: Elevated blood pressure (BP) at emergency department (ED) presentation and advancing age have been associated with risk of ischemic stroke; however, the relationship between BP, age, and transient ischemic attack/minor stroke (TIA/MS) is not clear.
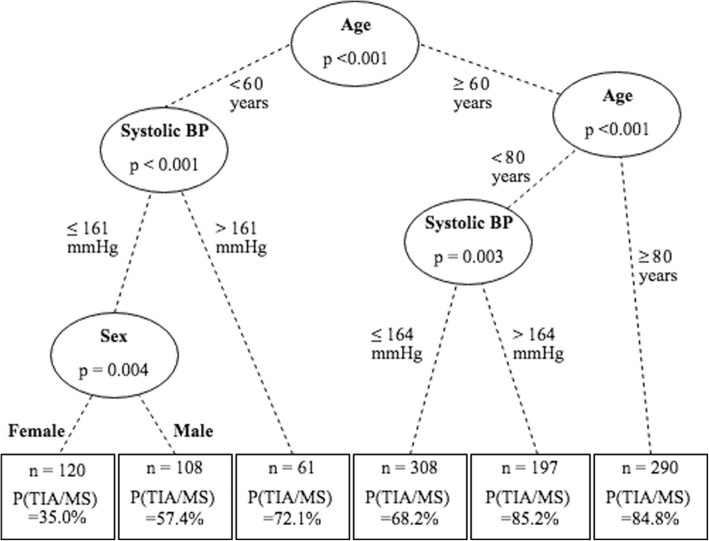
Methods: A multi-site, prospective, observational study of 1084 ED patients screened for suspected TIA/MS (symptom onset < 24 h, NIHSS< 4) between December 2013 and April 2016. Systolic and diastolic BP measurements (SBP, DBP) were taken at ED presentation. Final diagnosis was consensus adjudication by stroke neurologists; patients were diagnosed as either TIA/MS or stroke-mimic (non-cerebrovascular conditions). Conditional inference trees were used to define age cut-points for predicting binary diagnosis (TIA/MS or stroke-mimic). Logistic regression models were used to estimate the effect of BP, age, sex, and the age-BP interaction on predicting TIA/MS diagnosis.
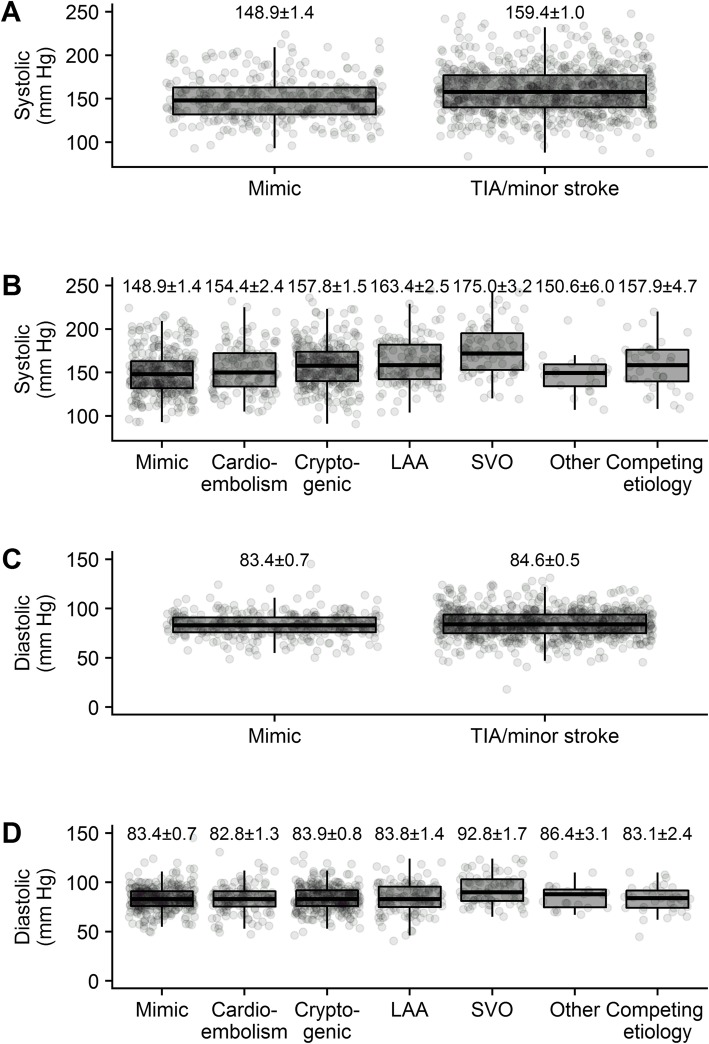
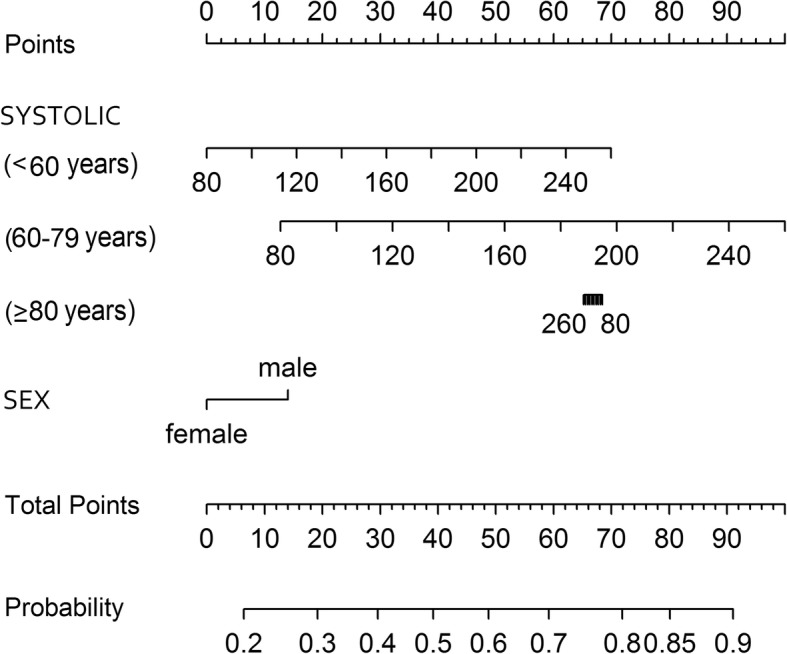
Results: Over a 28-month period, 768 (71%) patients were diagnosed with TIA/MS: these patients were older (mean 71.6 years) and more likely to be male (58%) than stroke-mimics (61.4 years, 41%; each p < 0.001). TIA/MS patients had higher SBP than stroke-mimics (p < 0.001). DBP did not differ between the two groups (p = 0.191). SBP was predictive of TIA/MS diagnosis in younger patients, after accounting for age and sex; an increase of 10 mmHg systolic increased the odds of TIA/MS 18% (odds ratio [OR] 1.18, 95% CI 1.00-1.39) in patients < 60 years, and 23% (OR 1.23, 95% CI 11.12-1.35) in those 60-79 years, while not affecting the odds of TIA/MS in patients ≥80 years (OR 0.99, 95% CI 0.89-1.07).
Conclusions: Raised SBP in patients younger than 80 with suspected TIA/MS may be a useful clinical indicator upon initial presentation to help increase clinicians' suspicion of TIA/MS.
Trial registration: ClinicalTrials.gov NCT03050099 (10-Feb-2017) and NCT03070067 (3-Mar-2017). Retrospectively registered.
Keywords: Blood pressure; Emergency medicine; Minor stroke; TIA; Transient ischemic attack.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Easton J, Saver J, Albers G, Alberts M, Chaturvedi S, Feldmann E, et al. Definition and evaluation of transient ischemic attack a scientific statement for healthcare professionals from the American Heart Association/American Stroke Association Stroke Council; Council on Cardiovascular Surgery and Anesthesia; Council on Cardiovascular Radiology and Intervention; Council on Cardiovascular Nursing; and the Interdisciplinary Council on Peripheral Vascular Disease. The American Academy of Neurology affirms the value of this statement as an educational tool for neurologists. Stroke. 2009;40(6):2276–2293. doi: 10.1161/STROKEAHA.108.192218. - DOI - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
