

Risk Factors and Incidence of Gastric Cancer After Detection of Helicobacter pylori Infection: A Large Cohort Study
- PMID: 31654635
- PMCID: PMC7010558
- DOI: 10.1053/j.gastro.2019.10.019
Risk Factors and Incidence of Gastric Cancer After Detection of Helicobacter pylori Infection: A Large Cohort Study
Abstract
Background & aims: Nearly all studies of gastric adenocarcinoma in the United States have relied on national cancer databases, which do not include data on Helicobacter pylori infection, the most well-known risk factor for gastric cancer. We collected data from a large cohort of patients in the United States to calculate the incidence of and risk factors for nonproximal gastric adenocarcinomas after detection of H pylori. Secondary aims included identifying how treatment and eradication affect cancer risk.
Methods: We performed a retrospective cohort study, collecting data from the Veterans Health Administration on 371,813 patients (median age 62 years; 92.3% male) who received a diagnosis of H pylori infection from January 1, 1994, through December 31, 2018. The primary outcome was a diagnosis of distal gastric adenocarcinoma 30 days or more after detection of H pylori infection. We performed a time to event with competing risk analysis (with death before cancer as a competing risk).
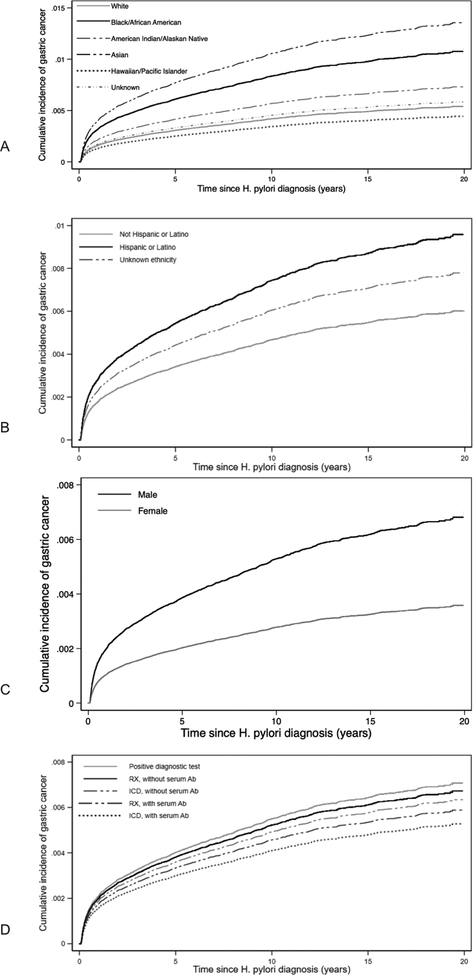
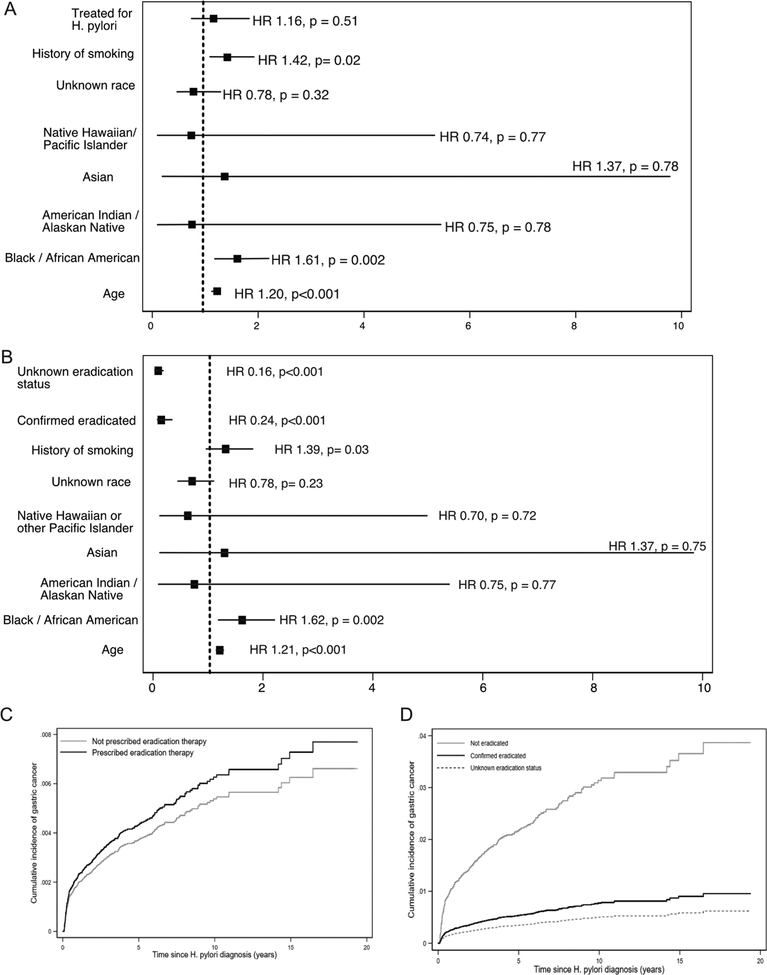
Results: The cumulative incidence of cancer at 5, 10, and 20 years after detection of H pylori infection was 0.37%, 0.5%, and 0.65%, respectively. Factors associated with cancer included older age at time of detection of H pylori infection (subhazard ratio [SHR], 1.13; 95% confidence interval [CI], 1.11-1.15; P < .001), black/African American race (SHR, 2.00; 95% CI, 1.80-2.22), Asian race (SHR, 2.52; 95% CI, 1.64-3.89) (P < .001 for race), Hispanic or Latino ethnicity (SHR, 1.59; 95% CI, 1.34-1.87; P < .001), and history of smoking (SHR, 1.38; 95% CI, 1.25-1.52; P < .001). Women had decreased risk of gastric adenocarcinoma compared with men (SHR, 0.52; 95% CI, 0.40-0.68; P < .001); patients whose H pylori infection was detected based on serum antibody positivity also had a reduced risk of cancer (SHR 0.74; 95% CI, 0.54-1.04; P = .04). Patients who received treatment for their H pylori infection still had an increased risk of gastric cancer (SHR, 1.16; 95% CI, 0.74-1.83; P = .51) but confirmed H pylori eradication after treatment reduced risk of gastric cancer (SHR, 0.24; 95% CI, 0.15-0.41; P < .001).
Conclusions: In a study of 371,813 veterans with a diagnosis of H pylori infection, we found significantly higher risks of gastric cancer in racial and ethnic minorities and smokers. Treatment of H pylori infection decreased risk only if eradication was successful. Studies are needed on the effects of screening high-risk persons and to identify quality measures for diagnosis, resistance patterns, and treatment efficacy.
Keywords: Antibacterial Therapy; Microbe; Screening; Stomach Cancer.
Copyright © 2020 AGA Institute. Published by Elsevier Inc. All rights reserved.
Figures

Comment in
-
One Step Forward But Room for Improvement in Reducing Risk of Gastric Cancer by Curing Helicobacter pylori Infection.Gastroenterology. 2020 Feb;158(3):466-467. doi: 10.1053/j.gastro.2019.11.008. Epub 2019 Nov 12. Gastroenterology. 2020. PMID: 31730770 No abstract available.
-
Risk Factors and Incidence of Gastric Cancer after Eradication of Helicobacter pylori.Gastroenterology. 2020 Jul;159(1):404-405. doi: 10.1053/j.gastro.2020.02.067. Epub 2020 Mar 28. Gastroenterology. 2020. PMID: 32234299 No abstract available.
References
-
- Jemal A, Bray F, Center MM, et al. Global cancer statistics. CA Cancer J Clin 2011;61:69–90. - PubMed
-
- Noone AM HN, Krapcho M, Miller D, Brest A, Yu M, Ruhl J, Tatalovich Z, Mariotto A, Lewis DR, Chen HS, Feuer EJ, Cronin KA (eds). SEER Cancer Statistics Review, 1975-2015, National Cancer Institute; Bethesda, MD.
-
- Wang F, Meng W, Wang B, et al. Helicobacter pylori-induced gastric inflammation and gastric cancer. Cancer Lett 2014;345:196–202. - PubMed
-
- Correa P Helicobacter pylori and gastric carcinogenesis. Am J Surg Pathol 1995;19 Suppl 1:S37–43. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
