

Uniportal video-assisted thoracic surgery reduced the occurrence of post-thoracotomy pain syndrome after lobectomy for lung cancer
- PMID: 31656663
- PMCID: PMC6790455
- DOI: 10.21037/jtd.2019.09.07
Uniportal video-assisted thoracic surgery reduced the occurrence of post-thoracotomy pain syndrome after lobectomy for lung cancer
Abstract
Background: Post-thoracotomy pain syndrome (PTPS) is difficult for thoracic surgeons to manage. PTPS should never arise after minimally invasive surgery (MIS). Uniportal video-assisted thoracoscopic surgery (U-VATS), a form of MIS for thoracic disease, has become more common around the world and might reduce the risk of PTPS after thoracic surgery. We compared the frequencies of PTPS after U-VATS-based and multi-port VATS (M-VATS)-based lobectomy for lung cancer.
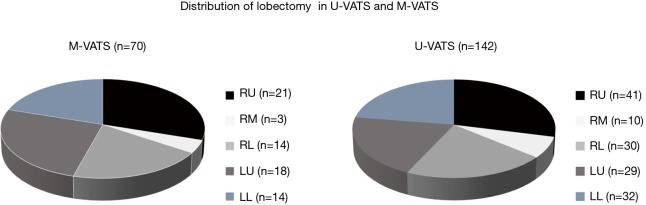
Methods: We compared the data for 142 and 70 cases in which U-VATS- and M-VATS-based lobectomies were performed, respectively. General surgical outcomes, the numeric rating scale (NRS) score, analgesic usage, and neuropathic pain according to the pain DETECT questionnaire (PDQ) were assessed. The presence of >1 of the following items at two postoperative months (POM) was used to diagnose PTPS: (I) an NRS score of >3, (II) analgesic use, and (III) exhibiting >1 of a list of 7 symptoms according to the PDQ.
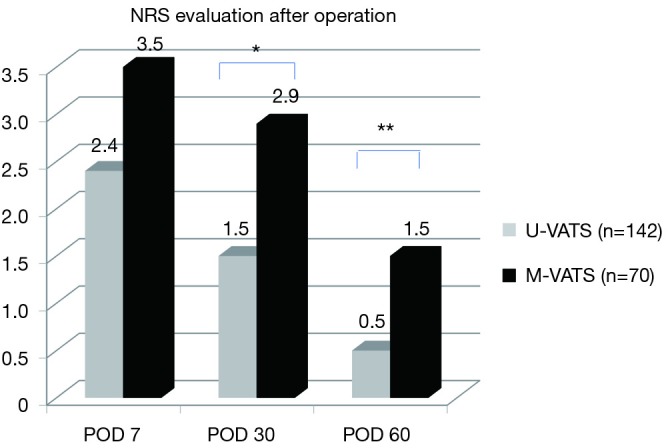
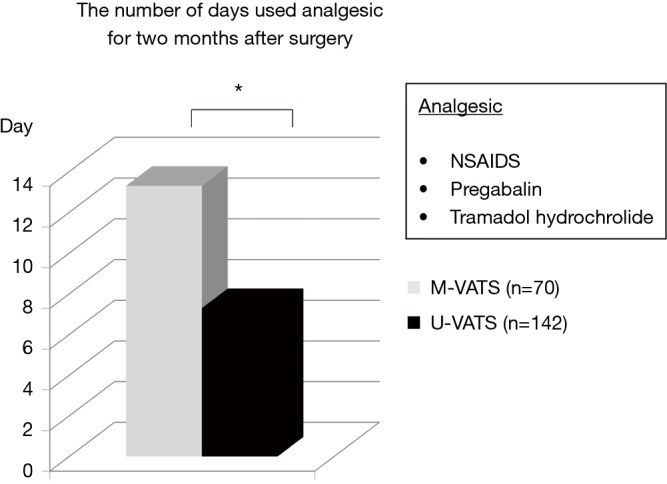
Results: There were no significant intergroup differences in the operation time, intraoperative blood loss, the number of dissected lymph nodes, or the duration of the drainage period or hospital stay. In the U-VATS and M-VATS groups, the mean NRS score during two postoperative months was 0.5±0.1 and 1.5±0.3, respectively (P<0.01), and analgesics were used for a mean of 7.3±1.5 and 13.3±1.8 days, respectively, during the postoperative 2 months (P<0.01). As for the frequency of PTPS-related symptoms on postoperative month (POM) 2, allodynia (U-VATS: 2.1% vs. M-VATS: 10%, P=0.028), hypoesthesia (2.1% vs. 10%, P=0.028), and numbness (1.4% vs. 8.6%, P=0.029) often arose in both groups. PTPS occurred in 2.8% and 11.4% of the patients in the U-VATS and M-VATS groups, respectively (P=0.025).
Conclusions: Compared with M-VATS, U-VATS exhibited a significantly lower incidence of PTPS.
Keywords: Uniportal video-assisted thoracic surgery (U-VATS); early lung cancer; lobectomy; multiport VATS (M-VATS); post-thoracotomy pain syndrome (PTPS).
2019 Journal of Thoracic Disease. All rights reserved.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures


References
-
- Hirai K, Takeuchi S, Usuda J. Single-incision thoracoscopic surgery and conventional video-assisted thoracoscopic surgery: a retrospective comparative study of perioperative clinical outcomes. Eur J Cardiothorac Surg 2016;49 suppl 1:i37-41. - PubMed
-
- Shen Y, Wang H, Feng M, et al. Single- versus multiple-port thoracoscopic lobectomy for lung cancer: a propensity-matched study. Eur J Cardiothorac Surg 2016;49 Suppl 1:i48-53. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials