

Mortality Risk in Acute Ischemic Stroke Patients With Large Vessel Occlusion Treated With Mechanical Thrombectomy
- PMID: 31657277
- PMCID: PMC6898819
- DOI: 10.1161/JAHA.119.014425
Mortality Risk in Acute Ischemic Stroke Patients With Large Vessel Occlusion Treated With Mechanical Thrombectomy
Abstract
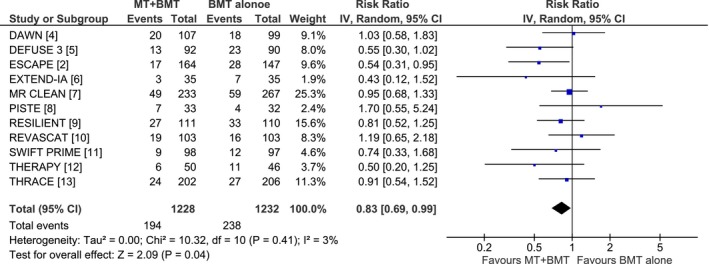
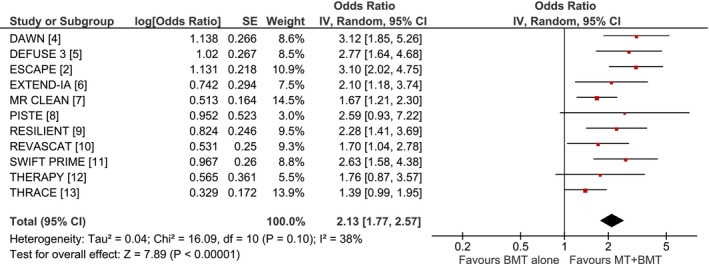
Background Recent randomized controlled clinical trials have provided solid evidence that mechanical thrombectomy (MT) coupled with best medical therapy (BMT) improve functional outcomes of acute ischemic stroke patients with large vessel occlusion compared with BMT alone. However, they provided inconclusive evidence on the benefit of MT on mortality. Methods and Results We evaluated the association of MT+BMT compared with BMT with the risk of 3-month mortality using aggregate data from all available randomized controlled clinical trials. We also sought to identify potential predictors on the mortality risk and performed univariate meta-regression analyses. Our literature search identified 11 eligible randomized controlled clinical trials, including a total of 2460 patients. The pooled rates of 3-month mortality were 15% (95% CI:12%-19%) and 19% (95% CI:16%-23%), respectively, in the MT+BMT and BMT groups. In the overall analysis MT+BMT was associated with a significantly lower risk for 3-month mortality compared with BMT (risk ratio=0.83, 95% CI:0.69-0.99; P=0.04), without heterogeneity across included studies (I2=3%, P for Cochran Q=0.41). No evidence of publication bias was present in funnel plot inspection and Egger statistical test (P=0.762). In meta-regression analyses no moderating effect on the aforementioned association was detected with patient age (P=0.254), sex (P=0.702), admission systolic blood pressure (P=0.601), admission glucose (P=0.277), onset-to-groin puncture time (P=0.985), administration of intravenous alteplase before MT (P=0.804), MT under general anesthesia (P=0.735), and successful reperfusion following MT (P=0.663). Conclusions Our meta-analysis provides evidence that MT+BMT reduces the risk of 3-month mortality compared with BMT alone. This association appears not to be moderated by individual patient or procedural characteristics.
Keywords: ischemic stroke; mortality; thrombectomy.
Figures
References
-
- Thrift AG, Thayabaranathan T, Howard G, Howard VJ, Rothwell PM, Feigin VL, Norrving B, Donnan GA, Cadilhac DA. Global stroke statistics. Int J Stroke. 2017;12:13–32. - PubMed
-
- Goyal M, Demchuk AM, Menon BK, Eesa M, Rempel JL, Thornton J, Roy D, Jovin TG, Willinsky RA, Sapkota BL, Dowlatshahi D, Frei DF, Kamal NR, Montanera WJ, Poppe AY, Ryckborst KJ, Silver FL, Shuaib A, Tampieri D, Williams D, Bang OY, Baxter BW, Burns PA, Choe H, Heo JH, Holmstedt CA, Jankowitz B, Kelly M, Linares G, Mandzia JL, Shankar J, Sohn SI, Swartz RH, Barber PA, Coutts SB, Smith EE, Morrish WF, Weill A, Subramaniam S, Mitha AP, Wong JH, Lowerison MW, Sajobi TT, Hill MD; ESCAPE Trial Investigators . Randomized assessment of rapid endovascular treatment of ischemic stroke. N Engl J Med. 2015;372:1019–1030. - PubMed
-
- Nogueira RG, Jadhav AP, Haussen DC, Bonafe A, Budzik RF, Bhuva P, Yavagal DR, Ribo M, Cognard C, Hanel RA, Sila CA, Hassan AE, Millan M, Levy EI, Mitchell P, Chen M, English JD, Shah QA, Silver FL, Pereira VM, Mehta BP, Baxter BW, Abraham MG, Cardona P, Veznedaroglu E, Hellinger FR, Feng L, Kirmani JF, Lopes DK, Jankowitz BT, Frankel MR, Costalat V, Vora NA, Yoo AJ, Malik AM, Furlan AJ, Rubiera M, Aghaebrahim A, Olivot JM, Tekle WG, Shields R, Graves T, Lewis RJ, Smith WS, Liebeskind DS, Saver JL, Jovin TG; DAWN Trial Investigators . Thrombectomy 6 to 24 hours after stroke with a mismatch between deficit and infarct. N Engl J Med. 2018;378:11–21. - PubMed
-
- Albers GW, Marks MP, Kemp S, Christensen S, Tsai JP, Ortega‐Gutierrez S, McTaggart RA, Torbey MT, Kim‐Tenser M, Leslie‐Mazwi T, Sarraj A, Kasner SE, Ansari SA, Yeatts SD, Hamilton S, Mlynash M, Heit JJ, Zaharchuk G, Kim S, Carrozzella J, Palesch YY, Demchuk AM, Bammer R, Lavori PW, Broderick JP, Lansberg MG; DEFUSE 3 Investigators . Thrombectomy for stroke at 6 to 16 hours with selection by perfusion imaging. N Engl J Med. 2018;378:708–718. - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
