

Global patterns of opioid use and dependence: harms to populations, interventions, and future action
- PMID: 31657732
- PMCID: PMC7068135
- DOI: 10.1016/S0140-6736(19)32229-9
Global patterns of opioid use and dependence: harms to populations, interventions, and future action
Abstract
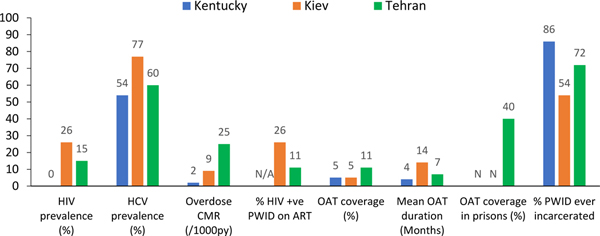
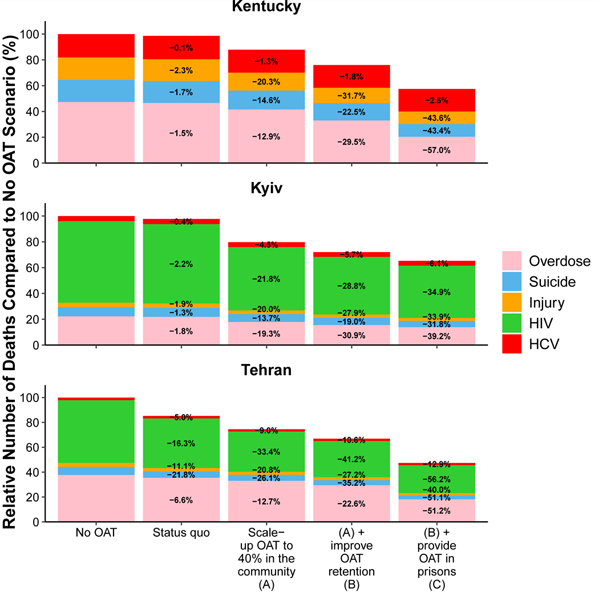
We summarise the evidence for medicinal uses of opioids, harms related to the extramedical use of, and dependence on, these drugs, and a wide range of interventions used to address these harms. The Global Burden of Diseases, Injuries, and Risk Factors Study estimated that in 2017, 40·5 million people were dependent on opioids (95% uncertainty interval 34·3-47·9 million) and 109 500 people (105 800-113 600) died from opioid overdose. Opioid agonist treatment (OAT) can be highly effective in reducing illicit opioid use and improving multiple health and social outcomes-eg, by reducing overall mortality and key causes of death, including overdose, suicide, HIV, hepatitis C virus, and other injuries. Mathematical modelling suggests that scaling up the use of OAT and retaining people in treatment, including in prison, could avert a median of 7·7% of deaths in Kentucky, 10·7% in Kiev, and 25·9% in Tehran over 20 years (compared with no OAT), with the greater effects in Tehran and Kiev being due to reductions in HIV mortality, given the higher prevalence of HIV among people who inject drugs in those settings. Other interventions have varied evidence for effectiveness and patient acceptability, and typically affect a narrower set of outcomes than OAT does. Other effective interventions focus on preventing harm related to opioids. Despite strong evidence for the effectiveness of a range of interventions to improve the health and wellbeing of people who are dependent on opioids, coverage is low, even in high-income countries. Treatment quality might be less than desirable, and considerable harm might be caused to individuals, society, and the economy by the criminalisation of extramedical opioid use and dependence. Alternative policy frameworks are recommended that adopt an approach based on human rights and public health, do not make drug use a criminal behaviour, and seek to reduce drug-related harm at the population level.
Copyright © 2019 Elsevier Ltd. All rights reserved.
Figures
Comment in
-
The global drug problem: change but not progression.Lancet. 2019 Oct 26;394(10208):1488-1490. doi: 10.1016/S0140-6736(19)32275-5. Epub 2019 Oct 23. Lancet. 2019. PMID: 31657726 No abstract available.
-
Older-age opioid-related deaths in the UK.Lancet. 2020 Jul 11;396(10244):94-95. doi: 10.1016/S0140-6736(20)30227-0. Lancet. 2020. PMID: 32653067 No abstract available.
References
-
- World Health Organization. WHO Model List of Essential Medicines. World Health Organization; 2017.
-
- World Health Organization. The ICD-10 Classification of Mental and Behavioural Disorders. Clinical descriptions and diagnostic guidelines. Geneva: World Health Organisation; 1992.
-
- World Health Organization. ICD-11 Beta Draft. 2016. http://apps.who.int/classifications/icd11/browse/l-m/en (accessed 4th November 2016).
-
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (Fifth Edition). Washington, DC: American Psychiatric Association; 2013.
Publication types
MeSH terms
Substances
Grants and funding
- R01 DA030762/DA/NIDA NIH HHS/United States
- R01 DA029910/DA/NIDA NIH HHS/United States
- R01 DA025943/DA/NIDA NIH HHS/United States
- P20 GM125507/GM/NIGMS NIH HHS/United States
- R01 DA033679/DA/NIDA NIH HHS/United States
- MR/K023233/1/MRC_/Medical Research Council/United Kingdom
- R01 DA030768/DA/NIDA NIH HHS/United States
- MR/K006525/1/MRC_/Medical Research Council/United Kingdom
- DP2 DA040236/DA/NIDA NIH HHS/United States
- R01 DA036975/DA/NIDA NIH HHS/United States
- K24 DA017072/DA/NIDA NIH HHS/United States
- R01 DA044170/DA/NIDA NIH HHS/United States
- R01 DA037773/DA/NIDA NIH HHS/United States
- R21 DA041953/DA/NIDA NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
